Publication scheme - information about the Trust
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust at a glance...
- Employ around 9,000 staff
- Mental Health and Disability Foundation Trust
- Local population of 1.7 million
- We work from over 70 sites across Cumbria, Northumberland, Newcastle, North Tyneside, Gateshead, South Tyneside, Sunderland and Middlesbrough
- 42% of staff (3,354 people) took part in the 2024 Staff Survey
- Inspected and rated Outstanding by the Care Quality Commission
- We also provide several regional and specialist services to England, Ireland, Scotland and Wales
- Part of the North East and North Cumbria Integrated Care Board (ICB)
- Turnover of around £647 million
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust 2024-25 in numbers...
- 8.6 (out of 10) based on feedback offered through Your Voice
- 43 - the average number of out of area bed days per month
- 1 of 8 - the number of mental health and disability trusts rated 'Outstanding' by the Care Quality Commission, out of 46 NHS Trusts
- 81.1% - the number of people with a first episode of psychosis beginning treatment with a NICE recommended care package within two weeks of referral
- 20.0% - the response rate to the 2024 Community Mental Health Survey, which is 0.2% lower than the previous year
- 80,139 - the number of service users cared for by the Trust on 31 March 2025
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust (CNTW) was formed in 2019 when the mental health and learning disability services in North Cumbria were transferred to Northumberland, Tyne and Wear NHS Foundation Trust.
We are one of the largest mental health, learning disability, autism, neurological, disability and specialist services organisations in the country and have an annual turnover of more than £611 million.
We provide a wide range of mental health, learning disability and neuro-rehabilitation services to a population of over 1.7 million people in North Cumbria and the North East of England. We employ over 9,000 staff, operate from over 70 sites and provide a range of comprehensive services including some regional and national services.
We support people in the communities of Cumbria, Northumberland, Newcastle, North Tyneside, Gateshead, South Tyneside and Sunderland working with a range of partners to deliver care and support to people in their own homes and from community and hospital-based premises. Our main hospital sites are:
- Northgate Hospital, Morpeth
- St George's Park, Morpeth
- St Nicholas Hospital, Newcastle Upon Tyne
- Walkergate Park, Newcastle Upon Tyne
- Ferndene, Prudhoe
- Monkwearmouth Hospital, Sunderland
- Hopewood Park, Sunderland
- Carleton Clinic, Carlisle
To focus on local populations and their needs we structure our services geographically into the following "Locality Care Groups"
- North - Northumberland and North Tyneside
- Central - Newcastle and Gateshead
- South - Sunderland and South Tyneside
- North Cumbria
What is the Quality Account?
All NHS healthcare providers are required to produce an annual Quality Account, to provide information on the quality of services they deliver.
We welcome the opportunity to outline how we have performed over the course of 2024-25, considering the views of service users, carers, staff and the public, and comparing ourselves with other Mental Health and Disability Trusts. This Quality Account outlines the good work that has been undertaken, the progress made in improving the quality of our services and identifies areas for improvement. To help with the reading of this document we have provided explanation boxes alongside the text, and some examples of service user and carer experience.
Statement of Quality from the Chair and Chief Executive
Welcome to our quality report. We are delighted to confirm that we have continued to make progress against our five strategic ambitions set in our Trust Strategy ‘With YOU in mind’. While 2024/25 has been another very challenging, but successful year for Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust (CNTW), our teams work together to deliver the highest levels of care.
We have continued to focus on improving service access, quality and productivity, while also making significant progress to transform how we deliver our care and support to those who need it and creating stronger foundations for the future. We want to build on all the good work we collectively delivered last year, and the progress made in improving the safety and quality of our services. Taking our strategy to the next step, our community transformation work will be critical to this, and we continue to develop and implement our model of care and support alongside our partners in primary care, the voluntary and charitable sectors and Local Authorities. This year we became a national pilot for the development of new models of community care and support, and we are rapidly developing the model in Whitehaven and Copeland in West Cumbria. This is our opportunity to go further faster.
We are absolutely committed to providing the highest standard of care and to achieve this we listen to the views of our service users and carers, our staff, our partners and other stakeholders.
Our aim is to make it easier for people to access care when they need it, to ensure the right organisations and people are involved at the right time, and that we have a joined-up approach to understanding and meeting people’s needs. The principles of our model of care and support apply across everything we do – they are grounded in humanity, respect for rights, partnership, continuity and fostering effective long-term relationships. By working with our partners to understand and meet the long-term needs of the people and communities that we serve, we think that we, in CNTW, will be better able to focus our efforts in delivering skilled therapeutic interventions, and ensuring that we have the people, knowledge and skills to deliver them well. We will test and develop this model wherever we can, in all that we do. We also want to make sure that we provide consistent, therapeutic and trauma informed care across our inpatient environments. If people need inpatient care, they need to feel safe and supported and that their rights are protected. We will relentlessly pursue our goal of reducing all forms of restrictive practice and
eliminating the use of coercive forms of restraint. We want to be an organisation that co-creates – that really values the views of the people and communities that we serve. We want to take the next steps in service user and carer involvement, so that it is deeply embedded in everything we do and in every decision that we make.
Our quality priorities are set by the Board and shaped by the views of everyone we work with and for. This report outlines those priorities for 2025/26 which you feel will best help us continue our journey to achieving our strategic ambitions. We want to thank everyone who has been, and continues to be, involved in the work reflected in this report, as we continue to work to improve our provision of safe and effective care for all who need us.
Statement from Executive Medical Director, Executive Director of Nursing, Therapies and Quality Assurance and Chief Operating Officer
In 2024-25 we have seen our staff, service users, carers and partners continue to work together to provide the best possible high-quality care underpinned by our trust strategy ‘With YOU in Mind’. We have continued to listen to our service users and their families, striving to achieve the best possible outcomes for people accessing our services and the Quality Account outlines our ongoing commitment to the delivery of compassionate person-centred care.
Our 5 Quality Priorities this year have been:
Implementation of the Patient Safety Incident Framework (PSIRF)
Delivering on key learning form key safety improvement themes;
- Reduce levels of restrictive practice
- Reduce levels of violence and aggression towards staff and patients
- Reduce levels of self-harm
- Improve the management of physical health care
Triangle of Care
Embedding learning through research ands informing improvements in care delivery
Embed a culture of Trauma Informed Care and its approaches across the
organisation.
Our staff have worked collaboratively with service users, carers, families and partners to make progress on these priorities, which is set out in detail in Part 2b of this Quality Account.
Learning from the improvements we have made with the Quality Priorities in 2024-25
we have refined the Trust’s Quality Aims and the underpinning goals, and we are delighted to present our new Quality Priorities for 2025-26 which are set out in Part 2a and will continue our commitment to work collaboratively to achieve outstanding outcomes.
Statement from the Lead Governor on the Quality Account
The Quality Account Report 2024/25 demonstrates the continued significant achievements the Trust has made over the last year, despite the challenges faced. In setting out the priorities for 2024/25, emphasis was placed on outlining the framework for the delivery of high-quality care and to include public accountability together with promoting quality improvements across the Trust. The Trust is committed to continuous improvement in all areas, and this is demonstrated by encompassing new technology, systems and procedures.
Quality data shared with Governors on a regular basis has demonstrated the drive for continuous improvement across the Trust. The comprehensive Quality Account Report which details the progress and delivery of quality priorities is welcomed by the Council of Governors. Public, Partner and Staff Governors continue to be active in all areas of the Trust, acting in an advisory capacity and by doing so, contributing to the strategic direction of the Trust. In addition, Governors act as ambassadors and as a link between the Trust and the communities we serve, by being represented on Committees and groups including:
- Resource, Assurance and Business Committee
- Quality and Performance Committee
- People Committee
- Audit Committee
- Charitable Funds Committee
- Mental Health Legislation Committee
- Governors Nomination and Renumeration Committee
- Service User Reference Group
- Bespoke groups driving forward service change
The Council of Governors receives regular updates on the progress being made throughout the Trust and continues to monitor the ongoing work of all concerned throughout the organisation. Frequent service visits are undertaken, seeing how services are run and hearing directly from patients and staff about their experiences provides assurance to the Council of Governors that patient needs are consistently being met. One example is the visit to the recently opened state-of-the-art secure facility ‘Sycamore’ which looks after men with a mental illness, learning disability or personality disorder who have entered the criminal justice system.
We are assured that there is a clear, continued focus on the quality improvement plan across Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust as we develop collaboration further with North East and North Cumbria ICB colleagues and Integrated Care System partners.
The Trust Strategy ‘With YOU in mind’ sets out five ambitions, underpinned by Trust commitments to service users, carers, staff and partners, co-produced by our stakeholders, that will help our teams to plan and take decisions, always ensuring that the focus remains on improving services for our community. We are excited about the future and about the improvements that closer working with others will bring to services for the benefit of all our community.
The Council of Governors want to take this opportunity to thank the Board of Directors and the dedication, commitments and compassion of our workforce, working within the Trust and the community in continuing to help and support those who need us in these challenging times.
Care Quality Commission (CQC) Findings
In 2018, the Care Quality Commission (CQC) conducted an inspection of our services and once again rated us as “Outstanding”. We are one of only eight Mental Health and Disability Trusts in the country to be rated as such, as of 1 April 2025.
During July and September 2024, the CQC assessed all wards for people with a learning disability or autism. At the time of writing this report the Trust had received the draft assessment report and was in the process of checking this report for factual accuracy.
In February 2025, the CQC conduced a focused inspection of community mental health and early intervention in psychosis teams. At the time of writing this report the Trust had not received the draft inspection report.
CQC Rating
The Trust was last rated 4th August 2022. Below are the headline ratings overall and ratings for the 5 domains. Read the full report here: Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust - Overview - Care Quality Commission (cqc.org.uk)
Overall rating - Outstanding
Are services
- Safe? Good
- Effective? Outstanding
- Caring? Outstanding
- Responsive? Outstanding
- Well-led? Outstanding
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust always aims to work in accordance with our values:
We are caring and compassionate... because that is how we'd want others to treat those we love.
We are respectful... because everyone is of equal value, is born with equal rights and is entitled to be treated with dignity. We want to protect the rights of future generations and the planet that sustains us all.
We are honest and transparent... because we want to be fair and open, and to help people make informed decisions.
Our Values
Our values are what bind us. We have considered these in the light of what people have asked of us. We believe that these are the values that we share together, and that we need to uphold if we are to meet our commitments.
Our strategy 'With YOU in mind' from 2023
We have developed long-term commitments in response to asks that developed during engagement, which will guide everything we do. We know that we are not currently achieving all these commitments – but we want them to be our guide. We want these commitments to be our inspiration for how we work and how we change over the years ahead.
Our aim is to deliver on these commitments every day, in every contact. In this document we set out how we will meet these commitments, through our vision, our values, and the ambitions that we are setting ourselves.
Commitment to our service users:
- Understand me, my story, my strengths, needs and risks. Work with me and others, so I can keep healthy and safe;
- Protect my rights, choices and freedom;
- Respect me and earn my trust by being honest, helpful and explaining things clearly;
- Support me, my family and carers in an effective, joined-up way that considers all my needs, and
- Respond quickly if I am unwell or in crisis, arranging support from people with the right expertise. Make sure I don’t have to keep repeating my story.
Commitment to our families and carers (also known as our 'Carers Promise')
- Recognise value and involve me.
- Listen to me, share information with me and be honest with me when there is information CNTW cannot share.
- Talk with me about where I can go for further help and information and let me know what I can expect from CNTW.
- Work with me to ensure we are all aware of my needs as a carer.
Commitment to our staff
- Respect me for who I am, trust me, value me and treat me fairly.
- Allow me freedom to act, to use my judgement and innovate in line with our shared values.
- Protect my time by making systems and processes as simple as possible so I can deliver the work I aspire to, learn, progress & get a balance between work & home.
- Offer me safe, meaningful work and give me a voice, working as part of a team that includes other professions and services, and
- Support me with compassionate managers who communicate clearly and understand what it’s like to do my job.
Commitment to our partners and communities
- Explain what to expect from CNTW.
- Help us to fight illness, unfairness and stigma.
- Make sure that organisations talk to each other and put the needs of people before their own. Share responsibility for getting things right.
- Get to know local communities. Respect their wisdom and history.
- Be responsible with public funds.
- Share our buildings, grounds and land.
- Protect the planet.
Our Vision
To work together, with compassion and care, to keep you well over the whole of your life.
Our Values
Our values are what bind us. We have considered these in the light of what people have asked of us. We believe that these are the values that we share together, and that we need to uphold if we are to meet our commitments:
We are caring and compassionate... because that is how we'd want others to treat those we love.
We are respectful... because everyone is of equal value, is born with equal rights and is entitled to be treated with dignity. We want to protect the rights of future generations and the planet that sustains us all.
We are honest and transparent... because we want to be fair and open, and to help people make informed decisions.
Trust overview of service users
Table 1 below shows the number of current service users as at 31 March 2025 by locality, and table 2 shows the total number of referrals in the year. Both tables have a comparison of the last 4 years.
Table 1: Service Users by locality 2021-22 to 2024-25 (data source: CNTW)
|
ICB Place Area |
2021-22 |
2022-23 |
2023-24 |
2024-25 |
|
NHS COUNTY DURHAM (TOTAL) |
1,288 |
1,373 |
1,454 |
1,584 |
|
DURHAM DALES, EASINGTON AND SEDGEFIELD |
573 |
606 |
641 |
698 |
|
NORTH DURHAM |
708 |
765 |
809 |
878 |
|
NHS NEWCASTLE GATESHEAD (TOTAL) |
16,731 |
18,584 |
21,454 |
25,091 |
|
GATESHEAD* |
5,640 |
6,516 |
7,820 |
9,642 |
|
NEWCASTLE* |
11,080 |
12,052 |
13,623 |
15,355 |
|
NHS NORTH CUMBRIA |
9,982 |
10,969 |
11,419 |
11,440 |
|
NHS NORTH TYNESIDE |
4,935 |
5,764 |
6,694 |
7,123 |
|
NHS NORTHUMBERLAND |
10,751 |
12,408 |
14,467 |
16,258 |
|
NHS SOUTH TYNESIDE |
5,114 |
5,652 |
6,154 |
6,301 |
|
NHS SUNDERLAND |
12,084 |
13,052 |
14,546 |
15,968 |
|
NHS TEES VALLEY (TOTAL) |
751 |
815 |
892 |
987 |
|
DARLINGTON |
153 |
166 |
169 |
189 |
|
HARTLEPOOL AND STOCKTON-ON- TEES |
278 |
313 |
362 |
409 |
|
SOUTH TEES |
315 |
334 |
360 |
388 |
|
Other |
785 |
920 |
932 |
924 |
|
Total |
62,421 |
69,537 |
78,010 |
85,676 |
*Note when Gateshead and Newcastle are separated a small number cannot be allocated too either
Table 2: Total referrals by locality 2021-22 to 2024-25 (data source: CNTW)
|
ICB Place Area |
2021-22 |
2022-23 |
2023-24 |
2024-25 |
|
NHS COUNTY DURHAM (TOTAL) |
2,666 |
2,843 |
2,910 |
3,040 |
|
NHS NEWCASTLE GATESHEAD (TOTAL) |
49,508 |
51,904 |
54,160 |
53,897 |
|
GATESHEAD |
18,303 |
19,818 |
20,839 |
20,838 |
|
NEWCASTLE |
30,344 |
32,035 |
33,258 |
32,854 |
|
NHS NORTH CUMBRIA |
43,961 |
44,817 |
46,964 |
42,640 |
|
NHS NORTH TYNESIDE |
19,280 |
18,710 |
19,019 |
17,761 |
|
NHS NORTHUMBERLAND |
35,519 |
37,729 |
37,805 |
35,094 |
|
NHS SOUTH TYNESIDE |
16,971 |
17,568 |
18,065 |
17,049 |
|
NHS SUNDERLAND |
46,612 |
43,584 |
44,272 |
41,574 |
|
NHS TEES VALLEY (TOTAL) |
764 |
754 |
858 |
919 |
|
Other |
2,356 |
2,471 |
2,810 |
2,555 |
|
Total |
217,637 |
220,380 |
226,863 |
214,529 |
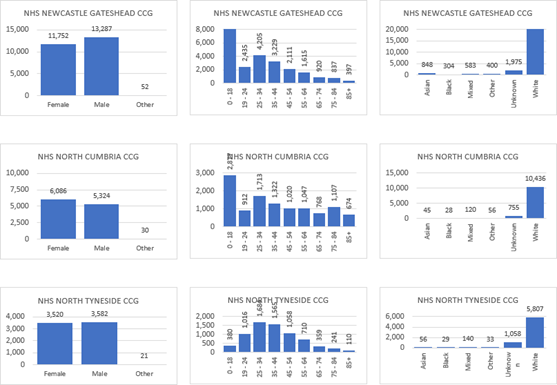
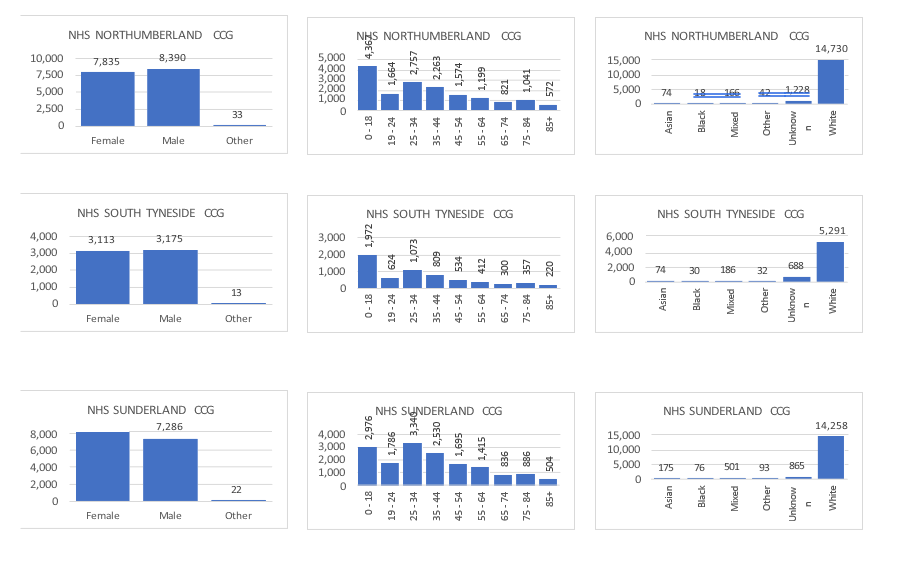
Breakdown of service users by age, gender, ethnicity
Graphs 1a-r: Gender, age and ethnicity breakdown of service users for our local ICB Place areas
This section of the report outlines the annual Quality Priorities identified by the Trust to improve the quality of our services in 2025-26.
Each year we set annual Quality Priorities to help us to achieve our long-term Quality Goals. The Trust identifies priorities in partnership with service users, carers, staff and partners from their feedback, as well as considering information gained from incidents and complaints, and by learning from Care Quality Commission findings.
CNTW will maintain commitment to progressing work across the previous 5 Quality Priorities including the Safety Themes and look forward to incorporating 2 more into our new Quality Aims:
- Continue to develop and embed a positive and safe culture.
- Improve physical health care.
- Reduce levels of restrictive practice and violence and aggression
- Reduce levels of self-harm
- Improve the care of people with a severe and enduring mental illness and/or physical disability.
To achieve these aims, the following priority areas have been identified:
- Strengthen communication with families and carers, ensuring they are actively involved in care decisions and when a patient deteriorates.
- Promote care planning that is person-centred, co-produced, and informed by the multidisciplinary team.
- Develop a consistent and evidence-based approach to risk assessment and safety planning across all services.
- Ensure safe and coordinated transitions between services.
- Improve the early recognition and response to deteriorating patients.
- Continue to improve sexual safety by reducing incidents and strengthening prevention and response.
- Improve handovers of care across inpatient services.
- Improve therapeutic engagement and observation across inpatient services.
- Manage and reduce the risk of cardiorespiratory arrest caused by sedative medication.
- Manage and reduce the risk of severe clozapine-induced constipation.
- Support staff wellbeing through increased access to resources, compassionate leadership, and healthy workplace culture.
Work in these areas will be reported on during 2025/2026, to provide a strong governance, assurance and oversight of delivery.
In this section we will review our progress against our 2024-25 Quality Priorities and consider the impact they may have made on each overarching Quality Goals.
How we did
Quality Priority 1
|
Quality Priority 1: Implementation of PSIRF (Patient Safety Incident Response Framework) |
Leads: Claire Thomas, Peter Astbury |
|
Summary of Progress |
|
|
|
|
Evidence of Impact |
|
|
|
|
Key Strengths |
|
|
|
|
Identified Areas for Development (Carried forward) |
|
|
|
Quality Priority 2
|
Quality Priority 2: Safety 5 Improvement Themes |
Leads: Claire Thomas (with individual leads per theme) |
|
Summary of Progress |
|
|
|
|
Evidence of Impact |
|
|
|
|
Key Strengths |
|
|
|
|
Identified Areas for Development (Carried forward) |
|
|
|
Quality Priority 2: Reducing Restrictive Practice
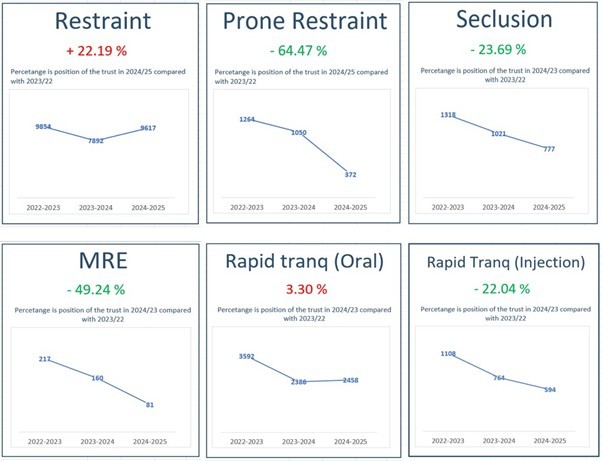
We can again report some encouraging reductions in 2024-2025 for the use of prone restraint. An ambitious target to eliminate the use of prone across the Trust has been agreed by the Trust Board. Alternative use of techniques to prone has resulted in increases within the restraint category.
The Positive and Safe team continues to be involved in a broad range of work across the trust. An overview of this year’s work follows:
The positive and safe team undertook a wholesale revision of the Trusts previous reducing restrictive intervention policy. The revised Reducing Restrictive Interventions and Violence Reduction Policy has now been ratified.
All inpatient teams will receive training relating to the policy throughout the year to ensure it is embedded within practice and further supports the Trusts ambition to reduce/eliminate both violence and restrictive practices.
A revision of the Trust wide Restraint Reduction meeting and governance has been implemented, with an increased focus on delivering ongoing reductions to restrictive practices, ensuring that care groups senior leaders’ expertise and experience is effectively utilised to support a strategic approach to reducing restraint.
Human rights awareness training has been delivered to all inpatient wards:
- Talk 1st is the trusts bespoke reducing restrictive interventions initiative and is entering its 8th year. We promote the use of Safewards and across all our inpatient wards.
- Each ward receives clinic visits from the Talk 1st team to support with action planning, scaffolding for teams, sharing good practice across the trust and any part of embedding Talk 1st initiatives.
- We encourage and support the use of data on both a ward and individual level to support in understanding distress, client view is also available for people to view their own data, with support, to promote better understanding of their own needs.
- Each ward attends quarterly Talk 1st cohort meetings these form the basis of the Trust ongoing quality cycle.
- Trauma informed care (TIC) the team have developed a training package which has been delivered during each team’s cohort meeting along with revised prompts within the team’s self-assessment tool to ensure TIC forms part of the ward’s quality initiatives.
- Annual Joint Conference with Tees Esk and Wear Valley Trust the sixth successful conference with over 200 delegates in attendance was held in 2024 with both national and trust staff providing some excellent and inspiring sessions during the day.
- Annual Report this year’s report is currently being completed and will be available in June.
- Quarterly insight reports the team continue to provide groups with interpretation of the relevant quarters trends as related to the application of restrictive interventions. Including cohort attendance from teams. The reports in future will be jointly produced between group and the positive and safe team.
- Post Graduate Certificate in reducing restrictive practice the course continues to develop and grow, a record number of staff applied this year with both internal and external candidates now taking part in this year's course.
- Long Term Segregation Panel the panel has supported and enhanced the HOPE(S) initiative, monitoring and providing advice/input to teams caring for patients within long term segregation and prolonged seclusion. A full day workshop was undertaken this year to refine and improve the work of the panel, the results from the day will inform future improvements to the work of the panel.
- The Talk 1st team continues to deliver bespoke training across the trust including:
- sensory training and scaffolding offered to teams as well as support revamping chill out rooms
- Pause training is a scenario-based training package.
- Safety huddle offers a quick and simple process asking, ‘Is the ward positive and safe?’ and ‘What can we do to make it better?’.
- Sleep Well is an initiate to improve sleep on inpatient wards, improving ward environments to be more conducive to a good night's sleep, offering psychoeducation sessions to improve sleep and a protected sleep period overnight where people are left undisturbed for people who are risk assessed as this being appropriate, sleepwell is currently being rolled out to all inpatient teams across the trust following board approval.
- Talk 1st awareness sessions.
Spotlight on HOPE(S)
HOPE(S) is a clinical model used to help individuals who are cared for in Long Term Segregation (LTS). The model is person centred, relentlessly positive and human rights based and looks to support teams to enhance the individuals’ quality of life whilst working towards ending the segregation. LTS is harmful to individuals causing emotional and physiological harm. Certain groups are particularly vulnerable to segregation use; autistic people and people with a learning disability representing around 95% of all individuals in segregation in England.
There is a national HOPE(S) team commissioned by NHS England and CNTW have established an internal lead role to support its ambition to significantly reduce and work towards ending segregation use.
National HOPE(S)
Independent research from Manchester Metropolitan University will be published in May 2025.
36 episodes of segregation ended in the North East and Yorkshire region through HOPE(S) intervention. 7 individuals in CNTW and their teams have received national HOPE(S) intervention. There is a regional community of practice and a national family network supporting families of individuals in segregation.
Average seclusion lengths in Trust
|
|
2018-19 |
2019-20 |
2020-21 |
2021-22 |
2022-23 |
2023-24 |
|
Time in hours |
37.00 |
74.51 |
89.91 |
79.85 |
64.53 |
54.63 |
*Whilst there is no way of directly attributing this to the work specifically around segregation such as HOPE(S), we do know that HOPE(S) directly communicates the critical period for harm to happen (48hours) and gives teams information on the need to reduce the length of seclusion.
CNTW HOPE(S)
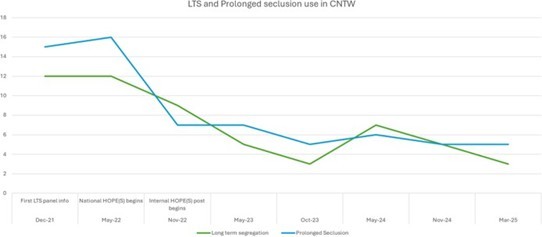
The HOPE(S) role has continued to support the embedding of the model within CNTW.
The graph below shows the reduction in segregation and prolonged seclusion use since introducing the role, the segregation panel and the national team.
- Supervision/ reflective practice support to teams on an ongoing basis.
- Practice sharing group/peer support for HOPE(S) trainers in place.
- Database of LTS cases and support provided including intervention targets.
- Review of prolonged seclusions or frequent seclusion users monthly. HOPE(S) lead will review case and offer support to teams proactively to prevent LTS use.
- Individualised in situ support.
- Seclusion policy revision to include HOPE(S) and bring trauma informed care and Human Rights to the forefront of the policy.
- Continued capturing of experiences and learning to share with others in training, Learning Improvement Group (LIG) etc.
Training and engagement
- 10 cohorts of staff trained in 2 day training to use the model. At least one session monthly for the next 3 months.
- Rolling HOPE(S) awareness sessions offered trust wide (1 session monthly)
- Engagement with key stakeholders; service user and carer reference group, boards, governor’s, advocacy, self-advocacy, estates.
- Peer supporter reflective practice monthly session.
- Lancaster University and Cumbria University have taken up the offer of HOPE(S) training and sessions have been delivered.
- HOPE(S) have supported 35 cases preventatively of LTS and none of these individuals went on to be in LTS.
|
Training Type |
CNTW March 25 |
|
Train the trainer programme – 5-day |
24 |
|
Barriers to Change Checklist - 2-day training |
347 |
|
Awareness training (3 hours) |
670 |
This represents a significant proportion of the national numbers in relation to HOPE(S) training.
LTS panel
All individuals in LTS in CNTW have had a Barriers to Change Checklist as part of HOPE(S) support to address Human Rights and work towards ending LTS and we are working to embed the process for reviews. All individual’s checklists should be reviewed at least 6 weekly. HOPE(S) practice informs LTS panel in trust – Human Rights focused.
How has the Improving the inpatient experience Quality Priority helped support the Safety Quality Goal of Keeping You Safe?
We aim to demonstrate success against this quality goal by reducing the severity of incidents and the number of serious incidents across the Trust’s services.
Table 3. Patient Safety incidents impact 2022-23 to 2024-25
|
Patient Safety Incidents by Actual Impact |
2022-23 |
2023-24 |
2024-25 |
|||
|
No Physical Harm |
16186 |
62.68% |
17364 |
61.91% |
25962 |
65.33% |
|
Low Physical Harm |
7584 |
29.37% |
8083 |
28.82% |
13042 |
32.82% |
|
Moderate Physical Harm |
1813 |
7.02% |
2299 |
8.20% |
448 |
1.13% |
|
Severe Physical Harm |
91 |
0.35% |
116 |
0.41% |
138 |
0.35% |
|
Fatal |
148 |
0.57% |
184 |
0.66% |
148 |
0.37% |
|
Total Patient Safety Incidents |
25822 |
100% |
28046 |
100% |
39738 |
100% |
The Trust continues to report its activity of patient safety incidents into the Learn From Patient Safety Events Service (LFPSE)
From April 2024, the grading of incidents was changed to reflect the national language of harm, and this is now used for all incidents within the Trust for both patient and staff activity. This grading is now used as standard and has been included for all incident data above.
The Trust continues to see an increase in the numbers of incidents reported into the national system since go live. This continues to be seen as a positive in our incident reporting culture, with still most incidents being reported as no physical and low physical harm incidents. As we move into 2025 / 26 there will be major development work to join the learning from the Patient Safety Incident Response Framework (PSIRF) investigations, linking them to the incidents that have been reported into the LFPSE, to join up national from local learning. There are also potential developments over the next year that will see organisations having a greater focus on staff related activity with the potential to report violence against staff information into national systems.
Degree of harm in incident reports
The following categories are used across the NHS for patient safety incident reports:
No Physical Harm - a situation where no physical harm occurred: either a prevented patient safety incident or a no physical harm incident.
Low Physical Harm - Minimal harm occurred - patient required extra observation or minor treatment. Did not or is unlikely to need further healthcare beyond a single GP or A&E visit. Did not or is unlikely to need further treatment beyond dressing changes or short courses on oral medication.
Moderate Physical Harm - Has needed a likely to need healthcare beyond a single GP or A&E visit and beyond dressing changes or short courses of medication, but less than two weeks additional inpatient care and/ or less than 6 months of further treatment and did not need immediate life-saving intervention.
Severe Physical Harm - Permanent harm/ permanent alteration of the physiology needed immediate life-saving clinical intervention, likely to have reduced the patient's life expectancy.
Fatal, Death - any unexpected or unintended event that caused the death of one or more patients.
Table 4: Total incidents 2024-25 by local authority, includes patient safety and non- patient safety incidents
|
Place |
No Physical Harm |
Low Physical Harm |
Moderate Physical Harm |
Severe Physical Harm |
Fatal Harm |
Total |
|
Cumbria |
5822 |
2186 |
99 |
20 |
279 |
8406 |
|
Gateshead |
5117 |
1704 |
97 |
12 |
86 |
7016 |
|
Newcastle North and East |
4592 |
2168 |
134 |
18 |
156 |
7068 |
|
Newcastle West |
4029 |
1360 |
151 |
13 |
133 |
5686 |
|
North Tyneside |
5904 |
2239 |
127 |
22 |
159 |
8451 |
|
Northumberland |
10980 |
4026 |
247 |
141 |
335 |
15729 |
|
South Tyneside |
5321 |
2886 |
143 |
10 |
157 |
8517 |
|
Sunderland |
6796 |
2908 |
148 |
25 |
307 |
10184 |
|
TOTAL |
48561 |
19477 |
1146 |
261 |
1612 |
71057 |
Data source: CNTW
Openness and Honesty when things go wrong: the Professional Duty of Candour
All healthcare professionals have a duty of candour which is a professional responsibility to be honest with service users and their advocates, carers and families when things go wrong. The key features of this responsibility are that healthcare professionals must:
- Tell the service user (or, where appropriate, the service user's advocate, carer or family) when something has gone wrong.
- Apologise to the service user. Offer an appropriate remedy or support to put matters right (if possible).
- Explain fully to the service user the short and long term effects of what has happened.
A key requirement is for individuals and organisations to learn from events and implement change to improve the safety and quality of care. As part of the Trust implementation of the Patient Safety Incident Response Framework (PSIRF), we have reviewed and updated our Incident policy and our Duty of Candour practice guidance note, using the new NHSE guidance engaging and involving patients, families and staff following a patient safety incident. Training is being developed to further raise awareness of the duty at all levels of the organisation.
Healthcare professionals must also be open and honest and take part in Patient Safety Incident reviews and investigations when requested. All staff are aware that they should report incidents or raise concerns promptly, that they must support and encourage each other to be open and honest and not stop anyone from raising concerns.
At CNTW we try to provide the best service we can. Unfortunately, sometimes things go wrong. It is important that we know about these so we can try to put things right and stop them from going wrong again. If you wish to make a complaint you can do so by post to: Complaints Department, St. Nicholas Hospital, Gosforth, Newcastle upon Tyne NE3 3XT
By email: complaints@CNTW.nhs.uk By phone: 0191 245 6672
Quality Priority 3
|
Quality Priority 3: Triangle of Care (ToC) |
Leads: Sarah Rushbrooke, Alane Bould |
|
Summary of Progress |
|
|
|
|
Evidence of Impact |
|
|
|
|
Key Strengths |
|
|
|
|
Identified Areas for Development (Carried forward) |
|
|
|
Quality Priority 4
|
Quality Priority 4: Research and Learning |
Leads: Simon Douglas |
|
Summary of Progress |
|
|
|
|
Evidence of Impact |
|
|
|
|
Key Strengths |
|
|
|
|
Identified Areas for Development (Carried forward) |
|
|
|
Quality Priority 5
|
Quality Priority 5: Embed Culture of Trauma Informed Care (TIC) |
Lead: Rebecca Courtney-Walker |
|
Summary of Progress |
|
|
|
|
Evidence of Impact |
|
|
|
|
Key Strengths |
|
|
|
|
Identified Areas for Development (To be carried forward 25/26) |
|
|
|
Assessment and Recommendations
|
Overall Assessment and Recommendations |
|
Strengths |
|
|
Key Risks and Gaps: |
|
|
Recommendations: |
|
Our feedback through the CQC Community Mental Health Survey
The Trust values the feedback from people accessing our Community Mental Health services. This survey is a good way of comparing ourselves with other similar Foundation Trusts and is a survey we have been involved in for over 20 years.
The summary below shows that the Trust performed better than expected across 5 survey questions. One question also scored much better than expected, which is equal best with 3 other Trusts. The trust performed about the same as other Trusts for 24 questions and did not perform worse than other Trust in any question.
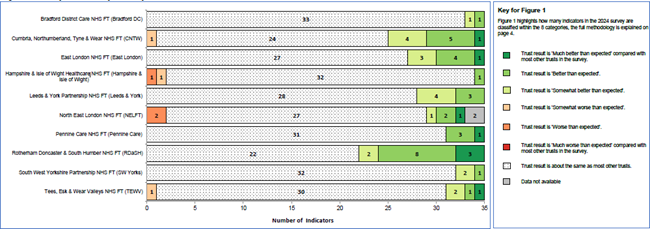
The table below shows the breakdown of how the Trust performed in each of the 13 sections, as well as the questions within those sections.
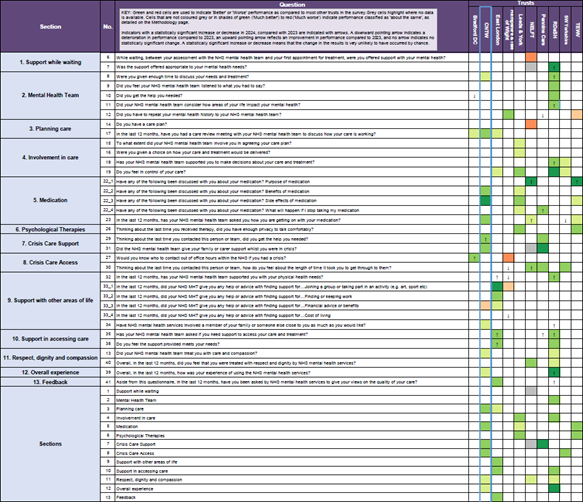
Table 5. CNTW performance for all questions and in comparison, to other Trusts
The question which scored much better than expected when compared to other Trusts was:
Question 22_3 ‘have any of the following been discussed with you about your medication? Side effects of medication?’
The 9 questions that offered us a score of better than expected related to:
- Service users having and being involved in the care planning process as well as being supported to make decisions about their care and treatment.
- Carers and close relative being involved in care planning.
- Services users being informed about their medication in areas such as the purpose, benefits and potential side effects.
- Service users feeling well supported in areas such as knowing who to contact outside of office hours if needed, being helped to access services and services helping to support people with physical health needs.
Performance against mandated core indicators
Patient experience of community mental health services' indicator score regarding a patient's experience of contact with a health or social care worker during the reporting period.
The Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust considers that this data is as described for the following reasons – this is an externally commissioned survey.
Table 6: Community Mental Health survey scores, 2019 to 2024
|
Health and social care workers |
2019 |
2020 |
2021 |
2022 |
2023 |
2024 |
|
CNTW |
7.7 |
7.6 |
7.3 |
7.1 |
7.1 |
7.2 |
|
National Average |
7.2 |
7.2 |
6.9 |
6.9 |
6.5 |
6.7 |
|
Highest national |
7.8 |
7.8 |
7.8 |
8.1 |
7.7 |
7.6 |
|
Lowest national |
6.2 |
6.1 |
6 |
6 |
5.7 |
5.9 |
|
Score out of 10, higher are better. Scores based on same two questions used in 2019 Data source: CQC |
|
|
||||
The Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust has taken the following actions to improve this score, and so the quality of its services by constantly engaging with service users and carers to ensure we are responsive to their needs and continually improve our services.
During 2022-23 the Trust has developed a ‘You Said – We Did’ poster resource for all wards and teams. This is built into the current Your Voice dashboard and supports each team to respond to the previous month’s feedback in a meaningful way, by discussing the major themes that have emerged during that month.
Importantly the ‘We Did’ section allows the team to say what will be done to respond to each theme as it develops.
During 2023-24 ‘You Said – We Did’ developed to become an important function for wards and teams. Continuing the good work that started in the previous year.
During April 2024 we moved from Points of You (PoY) to our new co-developed service user and carer experience survey Your Voice.
An update on our Service User and Carer Experience Survey - Your Voice
In April 2024 we moved to our new co-developed service user and carer experience survey Your Voice.
Some highlights from the first year of Your Voice are:
- 6,239 surveys were completed by service users and carers, 4,247 of these were completed by a service user and a further 576 were completed for a service user when they could not do this unaided. 1,206 surveys were completed by a carer. 210 surveys were completed where no option was chosen.
- 185 teams and wards received feedback in the year.
- The Friends and Family Test (FFT) score for the year was 8.6 out of 10, this score is around average when compared with mental health providers nationally. National average in January 2024 was 8.9.
- From April 2024 there have been 15,546 themed comments, of which, 74.1% were positive.
- The main themes discussed by service users and carers were Communications, Patient Care and Values and Behaviours.
- 624 You Said – We Did posters have been routinely produced.
In the last year, 6,239 surveys were completed by service users and carers. 4,247 of these were completed by a service user, 576 were completed by someone supporting a service user to share their experience, 1,206 were completed by a carer, relative or friend of a service user and 210 were completed by someone who shared an experience of a service without letting us know if they were a service user or a carer.
With the introduction of Your Voice, we took the opportunity to review how we could reach more service users and carers in a cost effective and environmentally friendly way opposed to just by mail. We now send a link for completion online via email and text and sending by mail is the last option we now use.
Between April 2024 – March 2025 we have sent:
- 13,344 emails
- 33,083 texts
- 10,642 letters
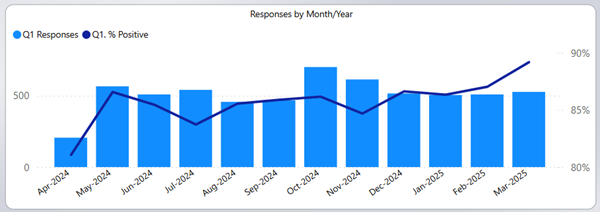
Question 1 of the Your Voice experience survey is the Friends and Family Test (FFT) question. This question is set by NHS England and all Foundation Trusts are required to ask it.
The question is: ‘Overall, how was your experience of our service?’, with the person answering from a set list of options from ‘Very Good’ to Very Poor’. Each chosen answer gives a score that leads to an average position over time.
The FFT question offers the Trust the opportunity to compare the overall satisfaction locally and with similar Trusts.
Question 1: Overall, how was your experience of the service?
6,119 responses were received with 85.9% stating they had a good or very good experience.
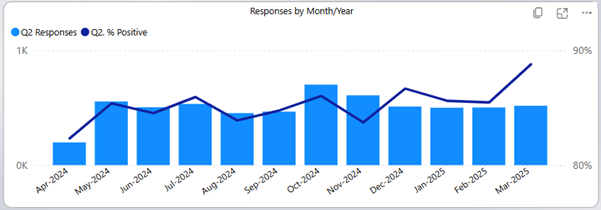
Question 2: How was the care we provided?
Overall, 6,046 responses were received with 5165 (85.4%) stating their care was very good or good.
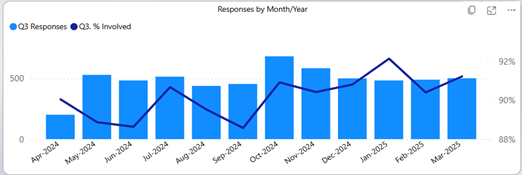
Question 3: How involved were you in your care?
Overall, 5,867 responses were received with 5294 (90.2%) stating they were very involved or somewhat involved.
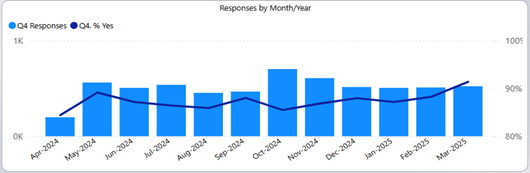
Question 4: Did you feel safe with our service?
6,091 responses were received to this question with 87.5% stating yes, they did feel safe.
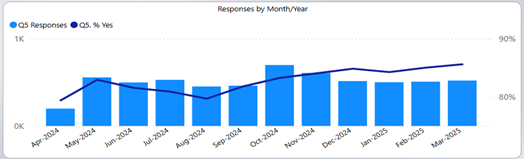
Question 5: Were you given information that was helpful?
6,052 responses were received to this question with 5,025 (87.5%) stating yes, they did receive helpful information.
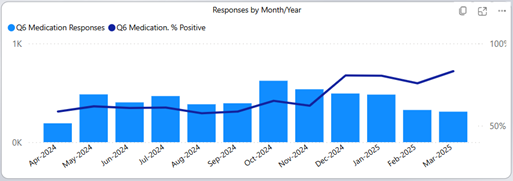
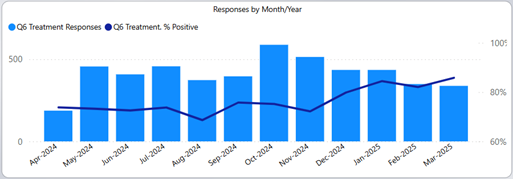
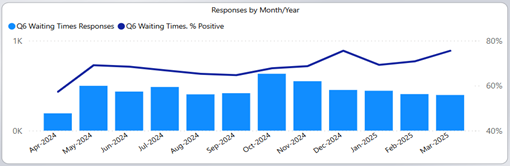
Question 6 is a three part question giving service users and carers the opportunity response to medication, treatment and waiting times.
Question 6: How did we do with medication?
5,091 responses were received with 66.1% stating they had a positive experience regarding medication.
Question 6: How did we do with Treatment?
4,936 responses were received with 76.0% positive response.
Question 6: How did we do with Waiting Times?
4,936 responses were received with 76.0% positive responses.
All question in the Your Voice experience survey offer the opportunity for service users and carers to share their experiences through a text box function. These comments are themed by the Commissioning and Quality Assurance team and included in a dashboard that all staff can access.
The comments as well as being themed into positive, negative and neutral are also assigned a main and sub-theme.
The most common theme for compliments has remained ‘Values and Behaviours’ across all years, with staff being ‘Kind/Caring/Friendly’ being the most discussed sub-theme of this main theme.
| Themes | Compliment | Negative | Neutral | Positive | ||||
| Category | % | Count | % | Count | % | Count | % | Count |
| Access to treatment or drugs | 4.2% | 27 | 27.1% | 176 | 6.9% | 45 | 61.8% | 402 |
| Admissions and discharges | 65.0% | 13 | 10.0% | 2 | 25.0% | 5 | ||
| Appointments | 29.7% | 110 | 14.3% | 53 | 55.9% | 207 | ||
| Clinical treatment | 19.9% | 27 | 9.6% | 13 | 70.6% | 96 | ||
| Communications | 1.5% | 74 | 15.5% | 743 | 8.1% | 388 | 74.9% | 3591 |
| Facilities | 3.5% | 27 | 21.7% | 168 | 6.1% | 47 | 68.7% | 532 |
| Other | 14.7% | 40 | 76.6% | 209 | 8.8% | 24 | ||
| Patient Care | 2.7% | 146 | 15.3% | 820 | 6.1% | 327 | 75.8% | 4052 |
| Prescribing | 0.3% | 1 | 27.0% | 84 | 26.4% | 82 | 46.3% | 144 |
| Privacy, Dignity and Wellbeing | 3.5% | 28 | 15.2% | 120 | 6.8% | 54 | 74.4% | 587 |
| Staff Numbers | 47.9% | 23 | 16.7% | 8 | 35.4% | 17 | ||
| Trust Admin/ Policies/ Procedures | 4.8% | 1 | 47.6% | 10 | 4.8% | 1 | 42.9% | 9 |
| Values and Behaviours | 4.1% | 135 | 5.7% | 190 | 1.5% | 49 | 88.7% | 2936 |
| Waiting Times | 44.7% | 335 | 12.1% | 91 | 43.1% | 323 | ||
| Total | 2.1% | 331 | 15.7% | 2439 | 8.1% | 1253 | 74.1% | 11523 |
Table 7. Main themes of comments 2024/25
Positive comments account for 11,523 of all comments or 74.1%. The main themes for these comments have been in relation to ‘Patient Care’, ‘Communications’ and Values and Behaviours’.
Neutral comments account for 1,253 of all comments or 8.1%. The main themes for these comments have been in relations to ‘Patient Care’ and ‘Communications’.
Negative comments totalled 2,439 or 15.7% of all comments themed. The most common theme related to Patient Care’, with 820 (15.3%) of all negative comments relating to this theme.
You Said - We Did
You Said – We Did (YSWD) is a monthly opportunity for teams to respond to the themes that emerged in the previous month. This happens through choosing a comment from a service user or carer that is representative of a dominant theme and responding as a team.
YSWD has been used informally by many wards and teams in the Trust for many years. A centralised system is available to all wards and teams to support being responsive to experience feedback as a monthly process.
The system is attached to the Your Voice dashboard and was designed to be a simple 2 step process that any staff member can carry out, without the need for ratio access.
YSWD is ‘Listen’ and ‘Do’ part of the NHS England » Ask Listen Do – feedback, concerns and complaints process that Your Voice supports. Something that the CQC are actively looking for evidence of during their visits. See the infographic below that explains the process and how Your Voice and YSWD fit into this process.
Complaints
Information gathered through our complaints process is used to inform service improvements and ensure we provide the best possible care to our service users, their families and carers.
Complaints have increased during 2024-25 with a total of 816 received. This is an overall increase of 37 complaints (5%) in comparison to 2023-24 and the highest number of complaints received per annum to date.
Table 8: Number of Complaints received 2022-23 to 2024-25
|
Financial Year |
Total |
|
2022-23 |
686 |
|
2023-24 |
779 |
|
2024-25 |
816 |
The Community Care Group accounted for 72% of the complaints received, followed by the Inpatient Care Group with 15% and the Specialist Care Group with 11%. The other 2% of complaints related to the non clinical directorates.
The three highest complaint categories: patient care, communication and values and behaviours:
- Patient care complaints increased by 10%
- Communications complaints increased by 4%
- Values and behaviours complaints decreased by 15%
Complaint categories which have significantly increased in comparison to 2023-24 are:
- Admissions and discharges complaints by 26%
- Appointments complaints by 28%
- Prescribing complaints by 42%
Complaint categories which have significantly decreased in comparison to 2023-24 are:
- Waiting times complaints by 19%
The Patient Advice and Liaison Service (PALS) gives service users and carers an alternative to making a formal complaint. The service provides advice and support to service users, their families, carers and staff, providing information, signposting to appropriate agencies, listening to concerns. We can also signpost complainants to local advocacy services who offer support and advice around making a complaint.
We now have access to the Interpreting Service and can request interpreters for complainants who are deaf or do not use English as a first language.
Table 9: Number of complaints received by category 2022-23 to 2024-25
|
Complaint Category |
2022/23 |
2023-24 |
2024-25 |
|
Patient Care |
180 |
193 |
214 |
|
Communications |
104 |
111 |
116 |
|
Values and Behaviours |
98 |
110 |
94 |
|
Admissions and Discharges |
53 |
55 |
74 |
|
Clinical Treatment |
43 |
47 |
42 |
|
Appointments |
31 |
26 |
36 |
|
Prescribing |
33 |
39 |
67 |
|
Trust Admin/ Policies/Procedures |
21 |
31 |
32 |
|
Access to Treatment or Drugs |
25 |
28 |
25 |
|
Other |
11 |
9 |
13 |
|
Facilities |
15 |
14 |
9 |
|
Waiting Times |
62 |
108 |
87 |
|
Privacy, Dignity and Wellbeing |
4 |
2 |
3 |
|
Restraint |
2 |
3 |
0 |
|
Staff Numbers |
2 |
1 |
2 |
|
Integrated Care |
0 |
0 |
0 |
|
Commissioning |
0 |
0 |
0 |
|
Consent |
1 |
1 |
2 |
|
Transport |
1 |
1 |
0 |
|
Total |
686 |
779 |
816 |
Data source: CNTW
Outcomes of complaints
Within the Trust there is continuing reflection on the complaints we receive, not just about the complaint but also on the complaint outcome. In 2024-25 we responded to complaints in line with agreed timescales in 94% of cases which is a 12% increase in comparison to 2023-24 and reflects the ongoing improvements made since the team staffing levels have been at full capacity.
Table 10: Number (and percentage) of complaint outcomes 2022-23 to 2024-25
|
Complaint Outcome |
2022-23 |
2023-24 |
2024-25 |
|||
|
Closed - Not Upheld |
168 |
24% |
195 |
25% |
236 |
29% |
|
Closed - Partially Upheld |
234 |
34% |
196 |
25% |
197 |
24% |
|
Closed - Upheld |
108 |
16% |
102 |
13% |
100 |
12% |
|
Complaint Withdrawn |
100 |
15% |
115 |
15% |
93 |
11% |
|
Decision Not to Investigate |
36 |
5% |
66 |
9% |
78 |
10% |
|
Still Awaiting Completion |
6 |
1% |
56 |
7% |
66 |
8% |
|
Unable To Investigate |
34 |
5% |
49 |
6% |
46 |
6% |
|
Total |
686 |
100% |
779 |
100% |
816 |
100% |
Data source: CNTW
Complaints referred to the Parliamentary and Health Service Ombudsman
If a complainant is dissatisfied with the outcome of a complaint investigation, they are given the option to contact the Trust again to explore issues further. However, if they choose not to do so then Stage 1 of the NHS complaints procedure has concluded. If they remain dissatisfied, they have the option to refer their complaint to the Parliamentary and Health Service Ombudsman (PHSO). This is known as Stage 2 of the NHS complaints procedure.
The role of the PHSO is to consider further independent investigation of complaints where individuals feel they have been treated unfairly or have received poor service from government departments and other public organisations and the NHS in England.
Activity during 2024-25 was as follows:
|
Table 11: Outcome of complaints considered by the PHSO |
Number |
|
Upheld |
1 |
|
Partially upheld |
3 |
|
Not upheld |
1 |
|
Decision not to investigate |
7 |
|
Investigation ongoing |
11 |
|
Total |
23 |
Data source: CNTW
NICE Guidance Baseline Assessments Completed 2024-25
The National Institute for Health and Care Excellence (NICE) provides national guidance and advice to improve health and social care. During 2024-2025 the Trust undertook the following assessments against appropriate guidance to further improve quality of service provided. Assessments were conducted against all published NICE guidance deemed relevant to the Trust.
1. NICE Baseline assessments undertaken in 2024-2025 compliant at baseline (6)
The following baseline assessments, undertaken in 2024-2025, were compliant at baseline and did not require action plan monitoring.
|
Ref. |
Topic |
|
NG 51 |
Suspected Sepsis: recognition, diagnosis and early management |
|
NG 191 |
COVID-19 Rapid guideline: managing COVID-19 |
|
QS 11 |
Alcohol-use disorders: diagnosis and management |
|
QS 207 |
Tobacco: treating dependence |
|
NG 214 |
Integrated health and social care for people experiencing homelessness |
|
NG 232 |
Head injury: assessment and early management |
2. NICE Guidance baseline assessments undertaken in 2024-2025 that require action plan monitoring (3)
The following baseline assessments are currently in action plan monitoring:
|
Ref. |
Topic |
Key Findings |
|
NG 181 |
Rehabilitation for adults with complex psychosis |
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 13.09.24. Deadline for fully implemented action plan:
The baseline assessment identified 124 recommendations relevant to CNTW. These recommendations were reviewed by a team of experts and there were 21 action points highlighted. The info below is a snapshot of this list.
|
|
Ref. |
Topic |
Key Findings |
|
|
|
staffed accommodation when there are early signs that placement may be breaking down
e.g. recurring admission, EIP patients who may have complex psychosis, those with forensic needs, transition from CYPS, physically frail, people who are out of area
|
|
Ref. |
Topic |
Key Findings |
|
|
|
|
|
QS 167 |
Promoting health and preventing premature mortality in black, Asian and other minority ethnic groups |
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 12.07.24 Deadline for fully implemented action plan: 31.03.25 Due to issues relating to the national process, the lead has asked to note an extension to 31.03.26
The Patient carer Race Equality Framework is currently in development and is expected to address some of the issues described above. NHS England has launched its first ever anti-racism framework: the Patient and Carer Race Equality Framework (PCREF), for all NHS mental health trusts and mental health providers to embed across England.
This mandatory framework will support trusts and providers on their journeys to becoming actively anti- racist organisations by ensuring that they are responsible for co-producing and implementing concrete actions to reduce racial inequalities within their services. It will become part of Care Quality Commission (CQC) inspections. The PCREF will support improvement in three main domains:
Trusts’ boards will be leading on establishing and monitoring concrete plans of action to reduce health inequalities
New data set on improvements in reducing health inequalities will need to be published, as well as details on ethnicity in all existing core data sets
Visible and effective ways for patients and carers to feedback will be established, as well as clear processes to act and report on that feedback. The anti-racism framework brings ground-breaking change to the sector, building on progress achieved locally, and promoting a whole new dimension of coproduction, where individuals and communities are at the heart of the design and implementation of the services they need. |
|
QS 13 |
End of Life Care for Adults |
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 10.03.24 |
|
Ref. |
Topic |
Key Findings |
|
|
|
Deadline for fully implemented action plan: 11.04.25
This baseline assessment demonstrates partial compliance and a moderate level of risk. Gaps in provision have been identified, specifically in training, education and awareness of the subject.
The provision of a 24-hour support service is not able to be provided. There are five quality statements relating to this baseline assessment; assessment demonstrated that CNTW were complaint in statements 1, 2, and 5. Statements 3 and 5 demonstrated partial compliance and the focus of the action plan.
There are actions underway due to other work being undertaken around this subject because of baseline assessment against NG142 End of life care for adults: service delivery and the participation in the recent National Audit of Care at End of Life
The aim of the training is to:
|
|
Ref. |
Topic |
Key Findings |
|
|
|
The plan is to now think about how this can be operationalised within older people’s services. 4. An increase in education as detailed in response to statement 3 would also help to reinforce the processes and documents available to support access to specialist palliative care advice out of hours. There are actions underway due to other work being undertaken around this subject as a result of baseline assessment against NG142 End of life care for adults: service delivery and the participation in the recent National Audit of Care at End of Life
|
3. NICE Guidance baseline assessment complete and action plan fully implemented in 2024-2025 (10)
|
Ref. |
Topic |
|
NG 204 |
Babies, children and young people’s experience of healthcare |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 26.09.22 Deadline for fully implemented action plan: 28.07.24 The action plan was fully implemented on 27.08.24 and signed off at CEC on 11.10.24 |
|
|
NG 53 |
Transition between inpatient mental health and community or care home settings |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 12.05.23 Deadline for fully implemented action plan: 01.09.24 The action plan was fully implemented on 03.02.25 and signed off at CEC on 14.03.25 |
|
|
NG 213 |
Disabled children and young people up to 25 with severe complex needs: integrated service delivery and organisation across health, social care and education |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 10.11.23 Deadline for fully implemented action plan: 15.05.24 The action plan was fully implemented and signed off at CEC on 11.10.24 |
|
|
NG 158 |
Venous thromboembolic diseases: diagnosis, management and thrombophilia testing |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 12.01.24 Deadline for fully implemented action plan: 07.05.24 The action plan was fully implemented and signed off at CEC on 11.10.24 |
|
|
QS 203 |
Brain tumours (primary) and brain metastases in adults |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 31.12.22 Deadline for fully implemented action plan: 31.07.24 The action plan was fully implemented and signed off at CEC on 11.10.24 |
|
|
QS 179 |
Child abuse and neglect |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 31.12.22 Deadline for fully implemented action plan: 01.07.24 The action plan was fully implemented on 12.11.24 and signed off at CEC on 13.12.24 |
|
|
NG 64 |
Drug misuse prevention: targeted interventions |
|
The action plan was fully implemented on 03.02.25 and signed off at CEC on 14.03.25 |
|
|
NG 227 |
Advocacy services for adults with health and social care needs |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 12.07.24 Deadline for fully implemented action plan: NA Approved with no specific action plan at BDG-Q on 04/03/2025. Signed off at CEC 14.03.25 |
|
NG 209 |
Tobacco: Preventing Uptake, Promoting Quitting and Treating Dependence (Update) |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 10.05.24 Deadline for fully implemented action plan: 01.10.24 The action plan was fully implemented on 01.10.24 and signed off at CEC on 11.10.24 |
|
|
QS 140 |
Transition from Children’s to Adult’s Services |
|
Initial Compliance: Partial Compliance Submitted for action plan monitoring: 01.05.24 Deadline for fully implemented action plan: 31.10.24 The action plan was fully implemented and signed off at CEC on 11.10.24 |
4. NICE Guidance baseline assessments undertaken prior to 2024-2025 that are currently in action planning (2)
The following baseline assessments are currently in action plan monitoring:
|
Ref. |
Topic |
|
NG 197 |
Shared decision making |
|
QS 139 |
Oral health in the community |
5. NICE Guidance baseline assessment in progress (7)
The following baseline assessments are currently underway within 2024-2025
|
Ref. |
Topic Details / Objective |
Date Published |
Current Deadline |
|
NG 23 |
Menopause: diagnosis and management |
14.03.25 |
tbc |
|
NG 116 |
Post-traumatic stress disorder |
16.01.19 |
30.04.25 |
|
NG127 |
Suspected neurological conditions: recognition and referral |
02.10.23 |
30.05.25 |
|
NG 216 |
Social work with adults experiencing complex needs |
26.05.22 |
31.05.25 |
|
NG 222 |
Depression in adults: treatment and management |
29.06.22 |
31.10.25 |
|
NG 236 |
Stroke rehabilitation in adults |
18.10.23 |
30.04.25 |
|
NG 248 |
Gambling-related harms: identification, assessment and management |
28.01.25 |
31.03.25 |
6. Statistical Information
|
NICE Baseline Category |
Total |
|
Compliant at Baseline 24-25 |
6 |
|
Action Plan Monitoring Required 24-25 |
3 |
|
Action Plan Fully Implemented 24-25 |
10 |
|
Action Plan Monitoring Pre 2024-25 |
2 |
|
In Progress as at 01.04.25 |
7 |
|
Total |
25 |
7. Rapid Quality Improvement Projects (RQIP) Completed 2024/2025
|
Community Care Group (56) |
||
|
1 |
RQIP-23-0119 |
Re- audit of prescribing standards within Newcastle and Gateshead Universal Crisis Team |
|
2 |
RQIP-23-0092 |
Re-audit of ECG monitoring of high dose methadone (>100mg) |
|
3 |
RQIP-23-0097 |
Audit on Clozapine Plasma Level and Annual Prescribing Reviews in North Northumberland CTT |
|
4 |
RQIP-23-0070 |
Audit of the transition of care process from child and young people to adult learning disability team |
|
5 |
RQIP-23-0047 |
Audit and evaluation of impact of co-occurring mental health difficulties and alcohol/substance misuse in Gateshead PLT A&E referrals |
|
6 |
RQIP-23-0059 |
Reaudit of physical health monitoring of young people prescribed medication for ADHD |
|
7 |
RQIP-24-0004 |
Audit of diagnosis of psychosis and or bipolar in an Older Adult Community Treatment Team to ensure appropriate family work interventions are offered. |
|
8 |
RQIP-24-0013 |
Advice And Guidance Evaluation, Re-Audit of Pilot |
|
9 |
RQIP-24-0039 |
Compliance with documentation of Consent to treatment in Patients on Community Treatment Orders in Newcastle and Gateshead Step Up hub team |
|
10 |
RQIP-24-0029 |
RE-Audit of quality and appropriateness of referrals to occupation therapy for assessment, diagnosis and management of Dementia within the Memory Protection Service |
|
11 |
RQIP-23-0027 |
Audit of referrals to NCASS |
|
12 |
RQIP-24-0026 |
Audit of annual side effect discussion with patients on clozapine in a sample of patients in community supported accommodation. |
|
13 |
RQIP-24-0045 |
Audit on the Comparison of Automatic and Manual Blood Pressure Monitoring in Children Prescribed Medication for Adhd and Its Impact on The Number of Gp/Cardiology Referrals Sent |
|
14 |
RQIP-24-0044 |
Audit to see if antipsychotic monitoring is up to date for patients open to EIP North Tyneside Team, abnormalities picked up, actioned and communicated to GP and Patient |
|
15 |
RQIP-23-0054 |
Understanding the experiences of young people and their families who receive a neurodevelopmental assessment from Sunderland CYPS. |
|
16 |
RQIP-24-0037 |
Audit on patient’s annual physical health monitoring against CNTW Trust’s Clozaril guidelines. |
|
17 |
RQIP-23-0095 |
Audit of GP shared care agreements is accepted or declined |
|
18 |
RQIP-24-0018 |
Audit on time from referral to assessment, length of assessment and proportion receiving diagnoses following changes made to referral process in 2017 |
|
Community Care Group (56) |
||
|
19 |
RQIP-24-0015 |
Audit to evaluate the quality of clinic letters sent to the GP by Medic staff (Consultants and SAS doctors), |
|
20 |
RQIP-24-0059 |
Audit to understand the Newcastle North-East Community Mental Health Team’s (NNECT) current valproate case load and assess if we were in compliance with the updated guidance. |
|
21 |
RQIP-24-0063 |
Audit of the Castleside Day Hospital QIP Pathway |
|
22 |
RQIP-24-0058 |
Audit of renal function tests prior to memantine initiation per BNF/NICE guidelines at the old age community setting. |
|
23 |
RQIP-24-0069 |
Assess if discharge letters from the crisis team are meeting RCPsych QNCRHTT standards. They should be sent to the GP, within 48 hours, with accurate medications. |
|
24 |
RQIP-24-0088 |
Re-Audit of time taken for implementation of changes to psychotropic medications to be actioned within general hospital. (original audit RQIP-21-0061) |
|
25 |
RQIP-24-0067 |
Audit of the monitoring of patients on antipsychotics. |
|
26 |
RQIP-24-0053 |
To assess if West Older People Community Treatment Team are complying with HDAT monitoring requirements |
|
27 |
RQIP-24-0046 |
Audit to see what is captured in MDT to try and Improve Documentation |
|
28 |
RQIP-24-0094 |
Re-audit of renal function tests prior to memantine initiation per BNF/NICE guidelines in the old age community setting. |
|
29 |
RQIP-24-0085 |
Audit of Patients Prescribed off-licence Psychotropic Medication in the Community Learning Disabilities Psychiatry Service |
|
30 |
RQIP-24-0064 |
Physical Health monitoring in children and young adults - SoTyne CYPS |
|
31 |
RQIP-24-0098 |
Analysing how well the Lester Tool is being completed in patients who are on depot anti-psychotics. |
|
32 |
RQIP-24-0071 |
Audit of clinic letters sent to GP following outpatient medical review at South Northumberland CTT. |
|
33 |
RQIP-24-0107 |
Audit of CYPS Non-Medical Prescriber (NMP) caseload with the ADHD clinic |
|
34 |
RQIP-24-0077 |
Audit on the Compliance with follow up protocol after discharge on Mowbray, Cleadon and Roker |
|
35 |
RQIP-24-0104 |
Advice And Guidance Evaluation, Re-Audit of Pilot |
|
36 |
RQIP-24-0066 |
Investigating Clozapine Induced Seizure prophylaxis with a focus on the use of Sodium Valproate. |
|
37 |
RQIP-24-0087 |
Audit of CYPS school-based clinic with the Intended purpose of doing school clinics for ADHD medication; |
|
38 |
RQIP-24-0096 |
Assessment of Electrocardiogram (ECG) monitoring and interpretation in patients within the North Cumbria Adult Eating Disorders Service |
|
Community Care Group (56) |
||
|
39 |
RQIP-24-0083 |
Baseline Audit on Antipsychotic Physical Health Monitoring and Initiation of Antipsychotic Treatment in Patients under a Community Treatment Team |
|
40 |
RQIP-24-0082 |
Evaluating Unlicensed / Off-label Medication Prescribing in the Sunderland North CTT |
|
41 |
RQIP-24-0073 |
Physical health assessment of new admissions by medical team for patients on Hadrian2 unit. |
|
42 |
RQIP-24-0115 |
Enhancing Conceptual framework of understanding of Risk Assessment: Multi-Professional Quality Improvement Activity by North Cumbria Crisis team |
|
43 |
RQIP-24-0074 |
Audit of documentation on CNTW Rio vs NUTH electronic patient record. Is information always being transferred between systems and how long does this take? |
|
44 |
RQIP-24-0076 |
Review of Newcastle Northeast Community Team Depot Administration Cards. |
|
45 |
RQIP-24-0025 |
Reaudit of -Palliative and End of Life Care in Dementia in Northumberland Older Persons Pathway LLCA-18-0039) Key words: Palliative care, end of life care. |
|
46 |
RQIP-24-0119 |
High Dose Antipsychotic Therapy Audit |
|
47 |
RQIP-24-0089 |
Embedding the Use of a Psychosis Rating Scale in the Early Intervention Psychosis (EIP) Team to Improve Patient Outcomes |
|
48 |
RQIP-24-0086 |
Audit on Transfer of Care from Newcastle and Gateshead Children and Young People’s Service Neurodevelopmental Team to Adult Neurodevelopmental Health Service. |
|
49 |
RQIP-24-0080 |
Audit of The Recording of Falls Risk Assessment in Old Age Community Patients |
|
50 |
RQIP-24-0055 |
NICE guidelines for ADHD assessment in SoTyne CYPS and the role of Qb test |
|
51 |
RQIP-24-0097 |
ECG monitoring in patients prescribed Antipsychotic medication |
|
52 |
RQIP-24-0036 |
Transition Referrals to the Adult ADHD Team via CYPS |
|
53 |
RQIP-24-0108 |
Re-Audit to see what is captured in MDT to try and Improve Documentation |
|
54 |
RQIP-24-0130 |
Re-audit of antipsychotic medication monitoring standards for adults with intellectual (learning) disabilities living in the community and under the care of the Adult Community Learning Disabilities Team (North Cumbria). |
|
55 |
RQIP-24-0132 |
Is anticholinergic burden assessed on referral to Older Age Psychiatric Liaison Team North Cumbria and monitored when mediation changes are made? |
|
56 |
RQIP-24-0139 |
Audit on Bowel Movement Monitoring and Proactive Measures in patients on Clozapine |
|
Inpatient Care Group (33) |
||
|
57 |
RQIP-23-0106 |
To ensure nursing/medical staff adequately completing physical health record at admission and updated every 6 weeks, in accordance with local policy |
|
58 |
RQIP-23-0130 |
Assessment of degree of compliance with 24-hour discharge summary standard from Hadrian Clinic inpatient wards in the February 2024 |
|
59 |
RQIP-23-0134 |
Audit compliance with substance misuse documentation on admission assessment |
|
60 |
RQIP-23-0136 |
ECG assessments following a new admission-a review on the compliance and challenges |
|
61 |
RQIP-23-0137 |
Prevalence of ear canal cerumen in older people’s psychiatric services |
|
62 |
RQIP-23-0120 |
Preferred Pain Scale to be used on the ward between DOLO PLUS and Abbey pain scale. |
|
63 |
RQIP-24-0001 |
Audit of preadmission process on Berwick Medium Secure Rehabilitation ward against QNFMHS standards |
|
64 |
RQIP-24-0023 |
Audit on Are staff on Harthope Ward meeting guidance regarding monitoring of weight for patients starting antipsychotic medication? |
|
65 |
RQIP-23-0121 |
Identifying the key factors that contribute to delayed discharges on a functional elderly adult psychiatric ward |
|
66 |
RQIP-23-0118 |
Patients who have been discharged from Oakwood Ward Carleton Clinic from January 2023 to December 2023 who have had a 72 follow up meeting arranged. |
|
67 |
RQIP-23-0062 |
Assessment of the pharmacological management of COPD on an inpatient dementia ward. |
|
68 |
RQIP-23-0114 |
Anaesthetic-ECT Time Interval: Is the time interval between admin of Propofol to the time of delivery of electricity for purpose of electroconvulsive therapy within limits set by the new AETI depart guideline. |
|
69 |
RQIP-23-0129 |
Monitoring constipation to prevent complications in the physical health of older people admitted to Mowbray Ward |
|
70 |
RQIP-24-0019 |
Re – audit of Review of progress notes entries in the older adult inpatient ward at Monkwearmouth Hospital. |
|
71 |
RQIP-24-0028 |
Are patients having their ECGs performed within 12 hours of admission, and if not is there a reason documented in RiO for non-compliance? |
|
72 |
RQIP-24-0003 |
Is Trust Policy Guidance being followed for Covert Medication as included in UHM-PGN003 being followed Ruskin Unit |
|
73 |
RQIP-24-0022 |
Monitoring of physical health observations for clozapine titration in PICU patients |
|
74 |
RQIP-24-0027 |
Audit of use of investigations in the assessment of dementia with reference to NICE guideline 97 |
|
75 |
RQIP-24-0040 |
Assessment and management of substance misuse in patients admitted with psychosis across inpatient working age male adult wards in St Georges Park Hospital. |
|
76 |
RQIP-24-0002 |
Re-audit of initial physical health assessment for patients admitted to the Rehabilitation ward measured against NICE guidance standards |
|
77 |
RQIP-24-0060 |
Audit of staff member involvement in MDT and Independent seclusion reviews within CAMHS PICU. |
|
78 |
RQIP-24-0047 |
Audit on the Adherence to Sodium Valproate Policy in Females of Childbearing Age |
|
79 |
RQIP-24-0033 |
Review of buccal midazolam care plans for epilepsy within inpatient secure services |
|
80 |
RQIP-24-0061 |
Audit to confirm if ECGs are done and documented for new admissions. |
|
81 |
RQIP-24-0062 |
Audit on the Physical examination on admission to an acute psychiatric unit. |
|
82 |
RQIP-24-0092 |
Re-audit on frequency of clinical reviews in Elm House |
|
83 |
RQIP-24-0100 |
Audit to assess compliance with trust guidelines around physical health monitoring, specifically in the use of NEWS2 scores in an old age inpatient psychiatry ward. |
|
84 |
RQIP-24-0101 |
Audit to monitor constipation to prevent complications in the physical health of older people admitted to Mowbray Ward |
|
85 |
RQIP-24-0049 |
Audit of self-administration of medicines in an older age acute functional ward. |
|
86 |
RQIP-24-0114 |
Re-audit to investigate the ward’s compliance to the Trust’s policy regarding the monitoring of patients on antipsychotic medications |
|
87 |
RQIP-24-0075 |
Audit on Recognising that patients with hypertension may not be having treatment titrated to target blood pressures and some diagnoses may be missed if no NEWS score |
|
88 |
RQIP-24-0109 |
Auditing the way capillary blood glucose is measured and recorded for inpatients on Warkworth ward (+/- other adult acute wards) who are taking insulin to manage their diabetes. |
|
89 |
RQIP-24-0110 |
Re-Audit of Compliance and Challenges in ECG Assessments for New Admissions in Fellside Ward |
|
Specialist Care Group (19) |
||
|
90 |
RQIP-23-0059 |
Reaudit of physical health monitoring of young people prescribed medication for ADHD |
|
91 |
RQIP-24-0030 |
Correspondence with relevant services and young people detailing outcomes of assessment within 1 week of initial assessment within the team. |
|
92 |
RQIP-23-0071 |
Care Plan Audit – review of care plans completed within the Regional Communication Aid Service against Trust standards. |
|
93 |
RQIP-23-0117 |
Physical health monitoring of young people prescribed Olanzapine within CYP-CEDS audited against CNTW Trust Policy (PPT-PGN-08). |
|
94 |
RQIP-23-0123 |
To check if clinicians adhere to in completing the required information on Regional Affective Disorder Services (RADS) questionnaire scoring sheet during patient assessments |
|
95 |
RQIP-23-0135 |
Re-Audit of RQIP-23-0056 for Cardiovascular monitoring with the use of acetylcholinesterase inhibitors in the Older Person’s Community Mental Health Services. |
|
96 |
RQIP-24-0034 |
Audit on the use of the risk assessment tool on RiO for patients referred to the CaPE clinic. |
|
97 |
RQIP-23-0076 |
Limitations of Medical Information Provided on Admission – Development and Implementation of a Preadmission Medical Triage Tool |
|
98 |
RQIP-24-0035 |
Psychotherapy waiting times to receive assessment and treatment |
|
99 |
RQIP-24-0056 |
An assessment of expected physical health monitoring associated with high-risk medications during inpatient admission |
|
100 |
RQIP-24-0057 |
Limitations of Medical Information Provided on Admission to Specialised Inpatient Neurorehabilitation – Closed-loop QIP Evaluation Following Implementation of a Preadmission Medical Triage Tool |
|
101 |
RQIP-24-0090 |
Audit of the Multiple Sclerosis Rehabilitation Clinic for Patients with Multiple Sclerosis at Walkergate Park. |
|
102 |
RQIP-24-0065 |
Audit of the number of patients who DNA appointments at the Forensic Community Service from Oct 2023 to Oct 2024. |
|
103 |
RQIP-24-0079 |
An audit to assess the quality of the process of Category 3 referrals coming into Complex Neurodevelopmental Disorder Service (CNDS), measured against the standards of CNDS referral pathway protocol |
|
104 |
RQIP-24-0117 |
Review of the referral triage process for psychodynamic psychotherapy in the Newcastle Centre for Specialist Psychological Therapies |
|
105 |
RQIP-24-0121 |
Re-Audit of Preadmission process on Berwick Medium secure Rehabilitation ward against QNFMHS standards (Reaudit of RQIP-24-001) |
|
106 |
RQIP-23-0102 |
Audit of blood testing in NTaR drug and alcohol service |
|
107 |
RQIP-24-0135 |
Management of clozapine induced hypersalivation |
|
108 |
RQIP-24-0102 |
Audit of prescribing databases at Plummer court and review of prescribing database standards. |
Participation in National Clinical Audits
During 2024-25, 12 national clinical audits covered relevant health services that Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust provides.
|
Acronym |
Full Title |
|
NCAP |
National Clinical Audit of Psychosis |
|
NAIF |
National Audit of Inpatient Falls |
|
POMH- UK |
Prescribing Observatory for Mental Health-UK |
|
NAD |
National Audit of Dementia |
|
EIP |
Early Intervention in Psychosis |
|
NACEL |
National Audit of Care at the end of Life |
|
NAED |
National Audit of Eating Disorders |
The 12 national clinical audits eligible for participation by Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust during 2024-25 are shown in the table below (100% registration):
| National Clinical Audits 2023-24 HQIP Directory | |
| Carried forward from 2023-24 | |
| 1 | NA-23-104 Access Assessments for Admission to Adult Medium and Low Secure Services |
| 2 | NA-23-016.01 NAD Spotlight Audit: Community-Based Memory Services |
| 3 | NA-23-080.02 NAIF 23-24 |
| 4 | NA-23-084.02 NCAP EIP Re-Audit 23-24 |
| 5 | NA-23-084.01 NCAP New Process Pilot Audit 23-24 |
| 6 | NA-23-116 POMH-UK Topic 16: Rapid Tranquilisation |
| 7 | NA-23-101 POMH-UK Topic 22a: Use of medicines with Anticholinergic Properties in OP MH Service |
| 8 | NA-23-108 POMH-UK Topic 23a: Sharing Best Practice Initiatives |
| National Clinical Audits 2024-25 HQIP Directory | |
| New for 2024-25 | |
| 9 | NA-24-117 POMH-UK Topic 24a: Use of Opioids in Mental Health Services |
| 10 | NA-24-036.01 National Audit of Care at the End of Life |
| 11 | NA-24-125 National Audit of Eating Disorders |
| 12 | NA-24-068.01 POMH-UK Topic 18c: Use of Clozapine |
There were 5 national clinical audits that Cumbria, Northumberland, Tyne & Wear NHS Foundation Trust completed and closed in 2024-25
| National Clinical Audits | Cases submitted | Overall outcome | |
| 1 | NA-23-016.01 NAD: Spotlight Audit Community-Based Memory Services | 204 | Areas of concern |
| 2 | NA-23-084.02 NCAP EIP Re-Audit 23-24 | 378 | Minor areas of concern |
| 3 | NA-23-080.02 NAIF 23-24 | 3 (6) | Good practice |
| 4 | NA-23-101 POMH-UK Topic 22a Use of Anticholinergic Properties in Older Peoples Mental Health | 172 | Minor areas of concern |
| 5 | NA-123-108 POMH-UK Topic 23a Sharing Best Practice Initiatives | 5 | NA |
The reports for 5 national clinical audits were reviewed by the provider in 2024- 2025, and Cumbria, Northumberland, Tyne & Wear NHS Foundation Trust with the following agreed actions.
|
Project |
Actions |
|
|
1 |
NA-23-016.01 NAD Spotlight Audit: Community-Based Memory Services |
The key findings of the national audit show increases in waiting times overall, from referral to assessment and to diagnosis, but there is also a very wide variation between services in all areas of the audit. This includes waiting times, elements of assessment, diagnosis of dementia and subtypes, and post-diagnostic intervention.
The national report suggests that whilst the causes of such variation are not captured by the current audit data, this could include how individual services are set up (e.g. staffing, specialist input and variations in local commissioning) as well as factors such as the local referral rate, and how services record details (such as referral) in patient notes and the consistency of data entry/quality.
The national results demonstrate Areas of Concern. There is no risk rating for the national paper. All action plans will be developed locally within Memory Services and level of risk will be established in this way.
Localities developed action plans specific to their service and these were submitted for action plan monitoring on 31.10.24.
The re-audit is planned for Q4 25-26 |
|
Project |
Actions |
|
|
2 |
NA-23-084.02 NCAP EIP Re-Audit 23-24 |
NCAP continue to provide results to individual services and Trusts using a dashboard process. This allows EIP Teams to assess their compliance individually, and to compare outcomes from each service.
EIP Teams continue to develop individual action plans based on their results and this is added to the combined action plan for the national audit within CNTW. There are 8 domains that EIP Services are benchmarked against:
The results for CNTW demonstrated four areas in which ratings were maintained at top performing or performing well, with one improvement from performing well, to top performing.
The results demonstrated that there were two areas in which the Trust required improvements where previously the rating had been performing well.
This information resulted in the Trusts’ overall result changing from performing well, to needing improvement. This was difficult to understand, particularly as 5 domains out of 8 (62.5%) were rated as top performing.
The pilot audit of the proposed process, which was due to commence at the same time as the re-audit, was delayed at national level. It has recently been confirmed that this will be undertaken in Jun-25. A final report for the programme of audit that commenced in 2017 is due in Jul-25 |
|
3 |
NA-23-080.02 NAIF 23-24 |
Based on the work undertaken, and information provided by NAIF, the Trust is demonstrating Good Practice with a Low Level of Risk. |
|
Project |
Actions |
|
|
|
|
All wards where hip fractures occurred were 100% mental health wards. Nationally, this equated to 4%. There were 3 IFF cases reviewed for NAIF, with 100% of IFFs known to be as a result of a fall.
There continues to be issues relating to the identification of CNTW inpatient falls and, despite discussions and lists provided, does not appear to have been adequately addressed for the period of this audit. Our own records identify 6 hip fractures occurring within 2022 in comparison the National Falls audit data of 3 hip fractures.
There are several recommendations where there is no data to be reviewed. This is also an effect of the issues there is with identifying falls within the acute Trusts, and another example of how this audit does not provide enough information for it to be enough to provide assurance.
The process for 24-25 and onward is changing with the CNTW-relevant information able to be submitted directly to NAIF, and not through an acute trust. This change will benefit CNTW as it effectively takes away a barrier that has existed since the Trust agreed to participate. The Trust continues to participate in the national audit. |
|
4 |
NA-23-101 POMH-UK Topic 22a: Use of medicines with Anticholinergic Properties in OP MH Service |
This audit identified 172 eligible cases for collecting data from clients under the care of OA services across all 4 trust localities under the care of either inpatient or community services.
Key successes: Standard 1 related to the anticholinergic burden associated with prescribed antidepressant medicines OA. An antidepressant was prescribed in 88 of the audited cases, and in 91% (n=80) of these cases, an antidepressant with no or low anticholinergic burden was prescribed. Despite results showing non-compliance with the remaining audit standards, the level of compliance was encouraging, and areas of good practice were identified. Key concerns: Within the total sample, antipsychotic prescribing was identified in 107 cases, but only 65% (n=70) of these prescriptions were for agents with low or no anticholinergic burden. However, data for three-quarters of the total sample collected was from inpatient units where people with the |
|
Project |
Actions |
|
|
|
|
most severe mental illnesses are receiving care and treatment. It is possible therefore, that where antidepressants and antipsychotics with higher anticholinergic burden were prescribed, this was a considered choice after preferred medicines with less anticholinergic burden had provided insufficient therapeutic efficacy. Reassuringly, no antipsychotic medicines of high anticholinergic burden (AEC 3) were prescribed, and this was an improvement on the national sample.
Standard 2 assessed the prescribing of medicines for urinary incontinence. These medicines were prescribed in only 8 cases from the total audit sample. An agent with low or no anticholinergic burden was prescribed in 62.5% (n=5) cases, indicating non-compliance with this standard. It is unlikely that CNTW prescribers working in a specialist mental health setting would initiate or make changes to these medicines. These results are therefore unlikely to reflect prescribing practices within the trust. Although these results appear much worse than the national sample, the number of cases from the trust sample is too small to make any meaningful inferences from this result.
A degree of anticholinergic burden (i.e. AEC ≥1) was identified in 116 cases. An assessment of this anticholinergic burden (standard 3) was documented in 71% (n=82) of these. Of the cases where anticholinergic burden was assessed, 74% (n=61) of these used of a formal screening tool and the remainder (n=21) were assessed clinically. Although these results are non-compliant with the prescribed standard, they are significantly above the national sample and provides a solid foundation of practice on which to build upon in the action plan. Standard 3b assessed the screening of anticholinergic side effects associated with specific anticholinergic medicines (procyclidine, glycopyrronium, orphenadrine, hyoscine hydrobromide, trihexyphenidyl, pirenzepine and atropine drops). These medicines were prescribed in only 7 cases, and a review of side effects was documented in only 57% (n=4). This result is concerning, despite this being consistent with the results of the national sample. |
|
5 |
NA-23-108 POMH-UK Topic 23a: Sharing Best Practice Initiatives |
The aim of this QI programme was to highlight initiatives by Trusts to improve prescribing practice in mental health services, prompted by their participation in POMH QI programmes. Responses were reviewed and examples of practice changes have been included in a report produced to facilitate the sharing of such initiatives between Trusts, with |
|
Project |
Actions |
|
|
|
|
the potential to improve the quality of medication management. Recommendations from POMH-UK:
There are two factors emerge as making a positive contribution to the success of local enterprises:
The most common impediments to conducting QI activities were:
support these. |
Goals agreed with commissioners
Use of the Commissioning for Quality and Innovation (CQUIN) framework
The CQUIN framework aims to embed quality improvement and innovation at the heart of service provision and commissioner-provider discussions. It also ensures that local quality improvement priorities are discussed and agreed at board level in all organisations. It enables commissioners to reward excellence by linking a proportion of English healthcare providers' income to the achievement of local quality improvement goals.
Note that the CQUIN indicators are either mandated or developed in collaboration with NHS England and local Clinical Commissioners.
CQUIN Indicators
There were no CQUIN indicators for 2024-25.
Statement from the Care Quality Commission (CQC)
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust is required to register with the CQC and its current registration status is registered without conditions and therefore licensed to provide services. The CQC has not taken enforcement action against Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust during 2024-25.

External Accreditations
The Trust has gained national accreditation for the quality of services provided in many wards and teams.
Table 12: Current clinical external accreditations (31st March 2025).
|
External Accreditation |
Ward/Department |
Location |
|
Accreditation Programme for Psychological Therapies Services (APPTS) |
Sunderland Talking Therapies |
Monkwearmouth Hospital |
|
Electroconvulsive Therapy Accreditation Service (ECTAS) |
ECT Treatment Centre |
St George’s Park |
|
ECT Treatment Centre |
Hopewood Park |
|
|
Perinatal Quality Network (PQN) |
Beadnell |
St George’s Park |
|
Community Mental Health Team |
St Nicholas Hospital |
|
|
Quality Network for Community CAMHS (QNIC) |
Northumberland Children and Young People's Service |
St George’s Park |
|
Quality Network for Crisis Resolution and Home Treatment Teams (QN- CRHTT) |
Newcastle and Gateshead Crisis Resolution and Home Treatment Team |
St Nicholas Hospital |
|
Sunderland and South Tyneside Universal Crisis Team |
Hopewood Park |
|
|
Quality Network for Eating Disorders – inpatient and community (QED) |
Richardson Unit, Ward 31a |
Royal Victoria Infirmary |
|
Quality Network for Forensic Mental Health Services (QNFMHS) |
Tweed (Forensic Low Secure Unit) |
Northgate Park |
|
Tyne (Forensic Low Secure Unit) |
Northgate Park |
|
|
Alwinton |
Northgate Park |
|
|
Berwick |
Northgate Park |
|
|
Elsdon |
Northgate Park |
|
|
Harthope |
Northgate Park |
|
|
Linhope |
Northgate Park |
|
|
Rothbury |
Northgate Park |
|
|
Quality Network for Mental Health Rehabilitation Services (REHAB) |
Aldervale |
Hopewood Park |
|
Clearbrook |
Hopewood Park |
|
Quality Network for Older Adult Mental Health Services (QNOAMHS) |
Mowbray |
Monkwearmouth Hospital |
|
Roker |
Monkwearmouth Hospital |
|
|
Cleadon |
Monkwearmouth Hospital |
|
|
Akenside |
St Nicholas Hospital |
|
|
Oakwood |
Carleton Clinic |
|
|
Ruskin |
Carleton Clinic |
|
|
Quality Network for Inpatient Working Age Mental Health Services (QNWA) |
Longview |
Hopewood Park |
|
Shoredrift |
Hopewood Park |
|
|
Springrise |
Hopewood Park |
|
|
Quality Network - Learning Disabilities - QNLD |
Rose Lodge |
Hospital Drive, Hebburn |
|
Quality Network for Veterans Mental Health Services (QNVMHS) |
Op Courage Veterans Service |
Vermont House |
Data Quality
|
Clinical Record Keeping |
We will continue to monitor the use of the RiO clinical record system, learning from feedback and incidents, measuring adherence to the Clinical Records Keeping Guidance and highlighting the impact of good practice on data quality and on quality assurance recording. We will continue to improve and develop the RiO clinical record system in line with service requirements. We will improve staff awareness on the importance of good clinical record keeping through manager training sessions. |
|
CNTW Dashboard development |
We will continue the development and implementation of the new updated version of the CNTW dashboards, considering feedback from users, continuing to reflect on current priorities including the development and monitoring of new and shadow metrics that are introduced in line with national requirements and review current metrics. We will develop dashboards in line with the needs of the organisation. Established a rolling development plan with scheduled monthly updates. This will be accompanied by regular training sessions for staff so that they are informed of new changes and have access to training on ‘the basics’ of dashboard use. |
|
Data Quality Framework |
We will continue to develop and incorporate the data quality framework into the Trustwide information strategy to ensure the data quality score within the integrated performance report is applied consistently. We will also look to develop the framework within the CNTW dashboards and further develop a bespoke data quality dashboard. |
|
Mental Health Services Dataset (MHSDS) |
We will continue to understand and improve data quality issues and maintain the use of national benchmarking data. We will seek to gain greater understanding of the key quality metric data shared between MHSDS, and the Care Quality Commission. We will work with NHSE on data reconciliation so that internal reporting closely matches national reporting (where appropriate). We will improve our data maturity index score and understand areas where improvement is required including health inequalities data. We will improve the accuracy and recording of data in relation to protected characteristics. |
|
ICD10 Diagnosis Recording |
We will improve reporting on and diagnosis recording for service users with a learning disability and/or Autism, ADHD and dementia. |
|
Contract and national information requirements |
We will continue to develop quality assurance reporting to commissioners and national bodies in line with their requirements. We will produce and establish reporting via Integrated Care Systems to inform system level commissioning. |
|
Outcome Measures |
We will develop the current analysis of outcome measures focusing on implementing a system for reporting information back to clinical teams. We will improve outcome measure reporting by aligning it to appointment activities to evidence the impact interventions have on improvement. |
|
Electronic Staff Record (ESR) |
We will develop data quality monitoring of ESR data and develop action plans to address issues identified. We will continue to improve data quality with ESR to inform the Trusts ability in relation to workforce planning. We will introduce additional functionality from ESR to enable us to improve workforce planning. |
North East Quality Observatory (NEQOS) Retrospective Benchmarking of 2023-24 Quality Account Indicators
NEQOS provide expert clinical quality measurement services to many NHS organisations in the North East.
CNTW once again commissioned NEQOS to undertake a benchmarking exercise, comparing the Trust’s Quality Account 2023-24 with those of all other NHS Mental Health and Disability organisations. A summary of frequent indicators found in all Quality Accounts has been provided in Table 11:
Table 13: Nationally available Quality Account indicators for 2023-24
| Quality Account Indicators | England value | Peer median | CNTW | |
| 1 | Theme: Morale - NHS Staff Survey (2023) | 6.2 | 6.2 | 6.2 |
| 2 | Theme: Staff engagement - NHS Staff Survey (2023) | 7.1 | 7.2 | 7.1 |
| 3 | Workforce stability index, FTEs (%), March 2022 to March 2023 | 86.2 | 85.6 | 89.8 |
| 4 | National patient safety alerts actioned (%), 2022/23 | 62.0 | 100.0 | 100.0 |
| 5 | MHSDS Discharges followed up in 72 hours (%), Jan to March 2023 | 74.1 | 79.9 | 90.0 |
| 6 | Restrictive Interventions Data Quality Score, Jan to March 2023 | 91.1 | 79.3 | 83.9 |
| 7 | EIP patients treated within 2 weeks (%), March 2023 | 76.0 | 73.0 | 65.0 |
| 8 | Written complaints per 1000 FTEs, 2022/23 | 57.5 | 40.0 | 65.9 |
| 9 | People aged 18-69 in contact with MH services at the end of reporting period in settled accommodation (%) March 2023 | 19.0 | 25.5 | 22.0 |
| 10 | People aged 18-69 in contact with MH services at the end of the reporting period in employment (%) March 2023 | 5.0 | 5.0 | 5.0 |
Data source: North East Quality Observatory
Learning from deaths
The Serious Incident Framework (2015) continued to form the basis for the Trust’s Incident Policy which guided and informed the organisation about reporting, investigating, and learning from incidents including deaths during the majority of 2023-24. On January 22nd, 2024, the Trust transitioned from the Serious Incident Framework to the Patient Safety Incident Response Framework (PSIRF). PSIRF changes the way NHS Providers like CNTW report and respond to Patient Safety Incidents. As a result, CNTW reviewed and updated its incident review processes which are supported by the Trusts new PSIRF policy and Patient Safety Incident Response Plan (PSIRP). To note while PSIRF processes have been in place since January all reported deaths continue to be triaged for review by the Trusts dedicated Clinical Risk and Investigation department as they were under the previous framework.
During 2024-25, 1793 deaths were reported into the Trust’s Web based incident reporting system; this includes deaths identified through the NHS data spine portal. Of these, 1354 were recorded as natural cause deaths (75%). The total number of deaths is a slight increase from 1702 reported the previous year but in line with the 2022-23 period in which 1777 deaths were recorded.
The number of deaths in each of the Spring and Summer quarters was comparable and slightly less than the number of deaths in each of the Autumn and Winter quarters.
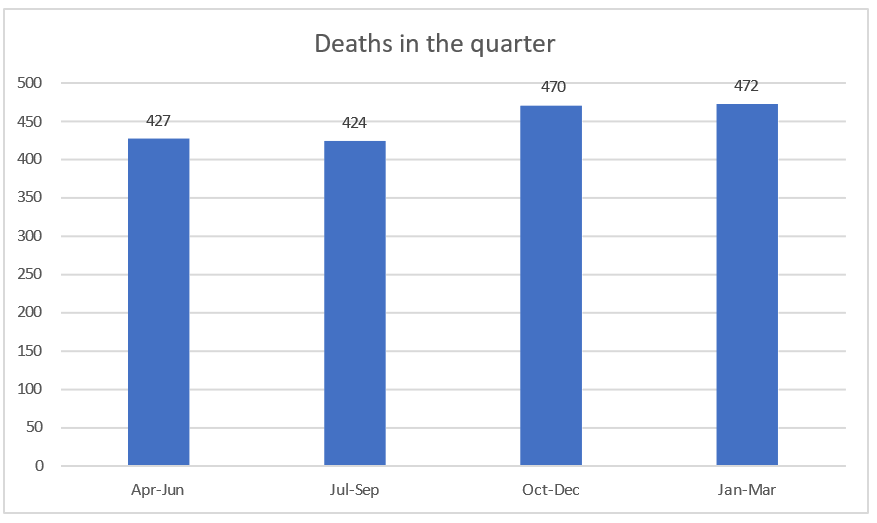
Processes to review deaths and promote learning
Following the introduction of the PSIRF framework in 2024, there have been changes in the level and type of reviews undertaken after deaths. Serious Untoward Incident (SUI) investigations have been replaced by Patient Safety Incident (PSI) investigations and the criteria for initiating such investigations have been changed. Therefore, the number of SUI investigations undertaken previously should not be compared with the number of PSI investigation currently completed.
The 72 hour reviews have been replaced by Early Learning Reviews (ELR) while After Actions Reviews (AAR) continue but with amended criteria for inclusion. Mortality Reviews (MR) have continued where natural cause deaths fulfil established criteria identified by the Royal College of Psychiatrists. Any single death may be escalated through two or more levels of review where this is appropriate to ensure that learning is identified and actioned.
During 2024-25 the following number and type of reviews were undertaken:
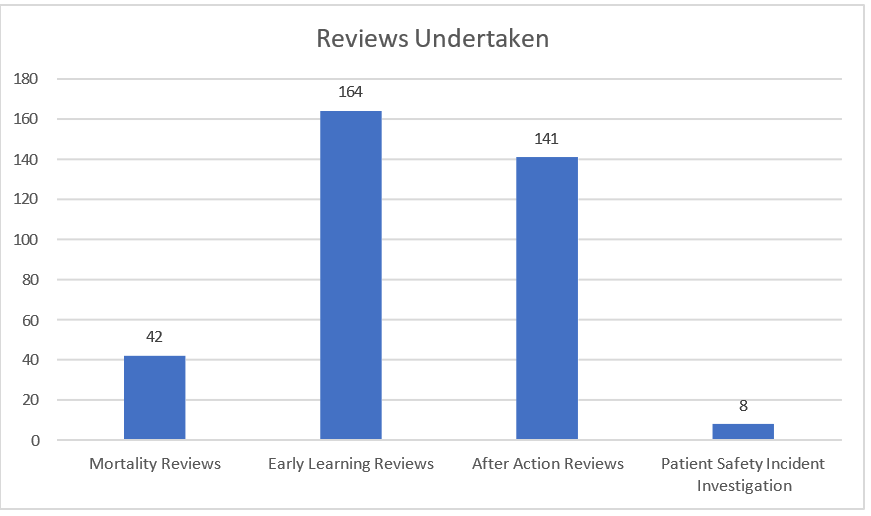
Owing to timescales involved in completing reviews a number of these remain live and are not yet complete at the time of writing. Similarly, several deaths that occurred towards the end of the previous financial year were completed in the early part on 2022-23. As a result, the summary of learning from reviews below results from completed reviews in 2023-24 as well as 2024-25.
The Trust has completed transition from the previous Serious Incident Framework to the new Patient Safety Incident Response Framework. This includes revision of the review processes as outlined above and the establishment of the Patient Safety Learning and Improvement Panel (PSLIP). Learning and Improvement webinars open to all staff are now firmly established, a steering group co-ordinates the content and delivery of the webinars.
We continue to report all deaths of people who are service users with an established diagnosis of learning disability and / or autism to the LeDeR (Learning from lives and deaths –people with a learning disability and autistic people) programme for further investigation. CNTW reported 72 deaths for LeDeR review between April 1st 2023 and March 31st 2024. Additionally, four of these deaths were also subject to a formal review process within the Trust.
Summary of learning from completed reviews
Over the last twelve months the Trust identified 1150 actions arising from 465 reviews. In 69 of the reviews there were no significant learning points identified. From the reviews undertaken in 2024-25 there were no deaths identified where it was more likely than not that the death was due to failure in the care process.
The top five themes which arose from the reviews were record keeping; care delivery; communication; clinical oversight and risk assessment.
The Trust has now embedded a new biopsychosocial risk assessment across services which is linked to the co-production of a safety plan with the service user, family and/or carers.
Learning from deaths has significantly impacted the development of the Trust safety and quality priorities for 2025-26.
NHS Number and General Medical Practice Code Validity
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust submitted records to the Mental Health Data Set. The position is at December 2024.
The percentage of records in the published data which included the patient’s valid NHS number was: 99.9%.
The percentage of records in the published data which included the patient’s valid General Medical Practice Code was: 99.9%
Data Security and Protection Toolkit attainment
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trusts DSPT 2023-24 submission was published on 30th June 2024 with all standards met. The deadline for the DSPT submission for 2024-25 is now the 30th of June 2025.
Clinical Coding error rate
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust was not subject to the Payment by Results clinical coding audit during 2024-25 by the Audit Commission.
Safe working hours for doctors in training
A report on safe working hours for doctors in training covering January to December 2024 was presented to the CNTW Trust board in January 2025.
The report is reproduced in Appendix 3.
Review of Quality Performance
In this section we report on the quality of the services we provide, by reviewing progress against indicators for quality improvement, including the NHS Oversight Framework, performance against contracts with local commissioners, statutory and mandatory training, staff sickness absence and staff survey results.
We have reviewed the information we include in this section to remove duplication and less relevant data compared to previous quality accounts. We have included key measures for each of the quality domains (safety, service user experience and clinical effectiveness) that we know are meaningful to service users, carers, our staff, our Council of Governors, commissioners and partners.
NHS Oversight Framework
Table 14: Self-assessment against the NHS Oversight Framework as at March 2025
|
|
Period |
Trustwide |
Newcastle/ Gateshead |
Northumberland |
North Tyneside |
South Tyneside |
Sunderland |
North Cumbria |
|
% in settled accommodation |
2024-25 |
51.9% |
56.4% |
58.3% |
42.2% |
58.1% |
60.3% |
36.6% |
|
% in employment |
2024-25 |
7.8% |
8.4% |
9.8% |
6.3% |
3.2% |
1.8% |
11.5% |
|
Cardio Metabolic |
||||||||
|
EIP |
31.03.2024 |
81.1% |
|
|
|
|
|
|
|
DQMI |
Dec 2024 |
93.7% |
|
|
|
|
|
|
|
IAPT Recovery |
March 2025 |
49.6% |
|
|
|
|
50.9% |
48.2% |
|
RTT% incomplete waiting less than 18 weeks |
2024-25 |
98.3% |
98.0% |
98.9% |
97.8% |
98.5% |
97.6% |
|
|
EIP |
2024-25 |
72.8% |
50.2% |
74.7% |
95.2% |
96.3% |
96.7% |
76.1% |
|
IAPT 6 Weeks |
March 2025 |
99.3% |
|
|
|
|
99% |
99.6% |
|
IAPT 18 Weeks |
March 2025 |
99.5% |
|
|
|
|
99% |
100% |
Performance against contracts with local commissioners
During 2024-25 the Trust had several contractual targets to meet with local authorities. Table 16 below highlights the targets and the performance of each local authority area against them for quarter four 2024-25 (1 January 2025 to 31 March 2025).
Table 15: Contract performance targets 2024-25 Quarter 4
|
Performance against contracts |
Newcastle / Gateshead |
Northumberland |
North Tyneside |
South Tyneside |
Sunderland |
N Cumbria |
|
Number inpatients followed up within 72 hours |
89.2 |
96.9 |
66.7 |
98.0 |
98.4 |
92.4 |
|
DTOCs |
11.9 |
9.4 |
11.0 |
22.7 |
9.7 |
18.2 |
|
RTT referrals waiting less than 18 weeks |
96.9 |
100 |
96.3 |
96.4 |
96.2 |
100 |
|
Valid NHS number |
100 |
100 |
99.9 |
100 |
100 |
100 |
|
Valid ethnicity |
92.0 |
92.2 |
82.8 |
89.1 |
93.5 |
92.2 |
|
Number of people who have completed IAPT Treatment |
|
|
|
|
52.2 |
49.3 |
|
EIP |
54.9 |
66.7 |
100 |
100 |
91.7 |
80 |
Statutory and Mandatory Training for 2024-25
It is important that our staff receive the training they need to carry out their roles safely. Each area has a trajectory in place to achieve the standard of 85% (the target for Information Governance was reviewed during 2024/25 and amended from 95% to 90%) in 2024-25.
Table 16: Training position as at 31 March 2025
| Stat and Mandatory Training | Position at 31/03/2023 | Position at 31/03/2024 | Position at 31/03/2025 |
| Fire Training | 86.90% | 87.90% | 90% |
| Health and Safety Training | 93.50% | 94.50% | 95.10% |
| Moving and Handling Training | 91.50% | 93.70% | 94.20% |
| Clinical Risk Training | 82.10% | 73.30% | 82.30% |
| Clinical Supervision Training | 80.30% | 79.30% | 82.30% |
| Safeguarding Children Training Level 1 | 95.30% | 96.30% | 95.70% |
| Safeguarding Children Training Level 2 | 82.8% | 91.30% | 91.20% |
| Safeguarding Children Training Level 3 | 79.10% | 86.10% | 87.50% |
| Safeguarding Adults Training Level 1 | 95.40% | 96.40% | 96.10% |
| Safeguarding Adults Training Level 2 | 87% | 93.80% | 93.8% |
| Safeguarding Adults Training Level 3 | 75.40% | 83.50% | 85.40% |
| Equality and Diversity Introduction | 94.20% | 95.20% | 95.70% |
| Hand Hygiene Training | 92.50% | 92.80% | 92.90% |
| Medicines Management Training | 83% | 61.40% | 76.40% |
| Rapid Tranquilisation Training | 77.20% | 68.30% | 73.20% |
| Combined MHA | 67.60% | 65.30% | 82.20% |
| Seclusion Training | 71.50% | 53.50% | 68% |
| PMVA Basic Training | 54% | 63.10% | 81.40% |
| PMVA Breakaway Training | 73.10% | 72% | 78.70% |
| Information Governance Training | 90.30% | 91.90% | 91.50% |
Data source: CNTW. Data includes CNTW Solutions, a wholly owned subsidiary company of CNTW.
Staff absence through sickness rate
High levels of staff sickness impact on service user care, therefore the Trust monitors sickness absence levels carefully.
Graph 1: Monthly staff sickness, CNTW and national, November 2022 to October 2024
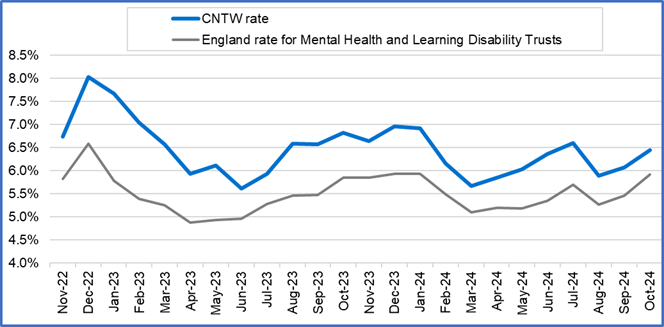
Graph 2: CNTW sickness rates 2024-25 against target, including position for 2023-24 and 2022-23
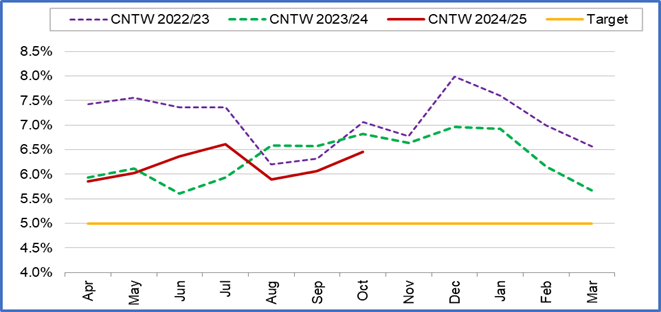
Data source: NHS Digital (data runs approx. 6 months behind actual). Data includes NTW Solutions, a wholly owned subsidiary company of CNTW.
Staff Survey 2024
The survey opened on 30 September 2024 and closed on 29 November 2024, an eight- week period for completion. There were 7950 members of staff were eligible to take part in the survey, 3354 staff completed the survey giving an overall response rate of 42%.
Following receipt and review of the 2024 staff survey findings, the Trust has begun identifying targeted initiatives to address areas requiring improvement and staff concerns. Some of these initiatives will build upon themes and programs of work already underway in response to the 2023 survey results alongside some new areas to consider which have emerged. Our actions are set out below.
As with the 2023 NHS Staff Survey this year was also opened to bank workers. 101 bank workers took part in the survey providing an overall response rate of 22% of the bank workforce. This is an improved response rate from the previous year of 20%.
We recognise the importance of our empowering our managers to view their results and determine local actions. Therefore, following the successful launch of the Staff Survey Dashboard in Spring 2024, there have been further developments to enable a localised review of results and actions as well as being able to compares results from previous years and across teams. Progress will be monitored through established local assurance groups. The bank worker survey results will also be available using this dashboard.
Transparency remains a core value. The 2024 results will be disseminated broadly across the organisation via a developed communication plan. This includes key findings presentations at Trust Board, People Committee, Council of Governors, Staff Side, and Corporate and Operational Directorate meetings.
The 2024 survey delivery was mixed mode. Our Inpatient services received paper survey, and all others received an electronic survey, whereby all staff received an email with a dedicated link to their individual survey.
The 2024 response rate was up 1 percentage point on our response rate of 41% in 2023. The 2024 median response rate for Mental Health and Learning Disability Trusts was 54%. This is the fourth consecutive year that we have a below average response rate. Our highest was 2018 when our response rate was 66.5% - the highest response rate in our comparator group.
Table 17: Staff Survey response rate 2021-2024
|
Response Rate |
2021 |
2022 |
2023 |
2024 |
|
Trust |
45% |
47% |
41% |
42% |
|
National Average (Mental Health/Learning Disability) |
52% |
50% |
52% |
54% |
From 2021 onwards, the results from questions are presented as per the elements of the People Promise. Scores for each element together with that of the survey benchmarking group Mental Health /Learning Disability Trusts which shows the Trust as above benchmark average in all areas are presented below:
Points of note
- The Trust is below average for all areas apart from ‘We are always learning’ and are the same as the average for morale.
- We have seen a decrease in all areas compared to the 2023 results.
- The People Promise is an area of focus in this year’s Operational Planning Guidance. We need to strive to embed these elements across the Trust and here is work already underway.
Graph 9: People Promise elements and themes
Actions
- Continued communication to staff from previous Staff Surveys around the themes of the People Promise (feedback into action)
- Line Manager guides and animations for initiatives relating to actions from results of the staff survey, flexible working, wellbeing, and retention (e.g. Stay Conversations)
- ESR project to strengthen reporting on flexible working and appraisal to enable ‘hot spots’ to identify additional support.
- Revised and updated Staff Survey Dashboard to enable full transparency of results and localised improvements.
- Review of our three main Employee Relations policies with a view to embedding a trauma informed approach and the ‘With YOU in mind’ values to create a compassionate culture
- Continue the work at the Trust Leadership Forum with a focus on culture and transformation.
- Development of a new violence and aggression risk assessment
- Launch of the new Leadership Development Programme and Management Skills Programme.
- Following the 2023 Staff Survey results and a review of the ED&I objectives and bullying survey we have relaunched the ‘Give Respect Get Respect’ campaign.
- The appointment of new Freedom to Speak up Guardians
Statement from Integrated Care Board (ICB), local Healthwatch and Local Authorities
Commissioner statement from NHS North East and North Cumbria Integrated Care Board (NENC ICB) for Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust Quality Account 2024/25.
NHS North East and North Cumbria Integrated Care Board (NENC ICB) is committed to commissioning high quality services from Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust (CNTWFT). NENC ICB is responsible for ensuring that the healthcare needs of patients that they represent are safe, effective and that the experiences of patients are reflected and acted upon. The ICB welcomes the opportunity to review and provide comment on this 2024/25 Quality Account.
Overview
The ICB would like to thank the Trust for the openness reflected in this year's Quality Account. The ICB would like to commend the staff for their commitment and dedication demonstrated throughout these challenging times and for striving to ensure that patient care continues to be delivered to a high standard. The ICB would also like to thank the Non- Executive Director for Quality and the Chief Nurse for welcoming the ICB to be a full member of the Trust's quality committee.
Achievements
The ICB would like to congratulate the Trust and its staff on the achievements made during this period. The ICB recognises the attainments detailed within the quality account, such as:
- Implementation of the Patient Safety Incident Response Framework (PSIRF) and the resultant journey in determining a robust approach to shared learning and improvement cycles.
- Violence reduction strategies, approaches to limiting long-term seclusion and promoting use of Safewards.
- The successful implementation of Your Voice in April 2024, and its continued development throughout the year. It was particularly pleasing to note the high percentage of positive comments received through this process during the year.
- The Trust producing over 600 You Said - We Did posters, demonstrating a strong commitment to listening and learning from feedback of service users and their families or carers.
- The expanding culture of research which is being embedded across the Trust.
Areas for further development
Now that the CQCs report for people with learning disabilities or autism has been published the ICB looks forward to monitoring the ongoing improvements and action plan that will be initiated in response. We will monitor progress through our ongoing attendance at the Trust quality committee.
We also recognise the further work outlined within the quality account to support full achievement of the 2024/25 priorities, in particular
- Qualitative and quantitative impact assessments,
- Risk assessments to drive change in clinical practice,
- Reducing the use of restrictive practice,
- Carer awareness training and
- Further lived experience integration.
Future priorities
The ICB is fully supportive of the identified Quality Priorities for 2025/2026 and welcomes the Trust’s commitment to continuing to embed processes and improvements across the quality priorities from the previous year along with the addition of new quality aims.
The ICB can confirm that to the best of their ability the information provided within the
annual Quality Account is an accurate and fair reflection of Trust performance for 2024/25. It is clearly presented in the required format, contains information that accurately represents the Trust's quality profile and aspirations for the forthcoming year.
NENC ICB remain committed to working in partnership with the Trust to assure the quality of commissioned services in 2025/26.
Yours sincerely,
Kate O'Brien
Director of Nursing, Mental Health, Learning Disabilities, Autism and Complex Care NHS North East and North Cumbria Integrated Care Board
Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust Quality Account 2024/25: Scrutiny Statement
Sunderland City Council
Sunderland City Council’s Health and Wellbeing Scrutiny Committee are again pleased to be able to provide a statement on Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust’s Quality Account.
The Committee continue to develop and maintain strong working relationships with all our health partners and remained focused on providing a critical friend challenge where appropriate, as well as representing the concerns of local people and communities in Sunderland.
The Committee are pleased to recognise the emphasis The Trust places on its commitments to families and carers, service users, staff, partners and communities all of which play an important part in The Trust’s delivery of quality services. These commitments become even more critical as we continue to see the integration of care and support at the local and neighbourhood levels, being able to understand and have the trust of local people and communities can only help to promote and develop this agenda.
In looking at the quality priorities for 25/26 Members are pleased to see that The Trust is continuing to develop and embed a positive and safe culture as well as looking to reduce the levels of harm through a safe and coordinated transition between services. Also, in improving the early recognition and response to deteriorating patients will help to improve outcomes for patients under the care of The Trust.
The Committee also acknowledges the extensive work detailed in the report in relation to the priorities set for 2024/25. It is positive to note the overall progress made in reducing the use of restrictive practices, and in particular the wholesale revision of The Trust’s policy on this issue. It is also good to see that this is to be followed up with all inpatient teams receiving updated training to support The Trust in its aims to reduce restrictive practices.
The Trust is also clearly committed to listening to and and learning from customer feedback and this highlighted throughout the report. The Committee recognises the work that has been undertaken to improve the patient experience based on customer feedback and a constant engagement with its service users. It is also positive to note that The Trust has also moved to a new service user and carer experience survey called Your Voice which provides further opportunities for customer engagement and service improvement.
The Health and Wellbeing Scrutiny Committee are also very interested in Men’s Mental Health with men less likely to seek help for mental health issues than women, it is important to raise awareness of men's mental health. Mental health issues can affect men in various ways, including depression, anxiety, and addiction. It can have a significant impact on their personal relationships, work, and overall quality of life. The Committee are interested in the services available for men in Sunderland and it is something that we intend to look at during the coming year.
The Health and Wellbeing Scrutiny Committee acknowledges that Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust remains committed to the delivery of safe and compassionate care for patients, and continues to work with partners, service users, stakeholders and regulatory bodies to achieve these aims. The Committee is therefore satisfied with the contents, identified priorities and endorses the Quality Report for 2024/25.
Cllr John Usher
Chair of the Health and Wellbeing Scrutiny Committee
Northumberland County Council
Statement from Northumberland County Council's Health and Wellbeing Overview Scrutiny Committee
The Health and Wellbeing Overview Scrutiny Committee Meeting is pleased to offer commentary for inclusion in the Quality Accounts for 2024/25. As an independent scrutiny committee, our role is to provide impartial assessment and insight into the planning, provision and operation of health services, acting as a critical friend to facilitate improvement.
In April, we devoted our work programme to reviewing the Quality Accounts of the local NHS Trusts. This approach allowed us to gain a comprehensive understanding of the healthcare landscape in Northumberland, enabling comparative analysis, trend identification, and benchmarking exercises.
Following our review of your Annual Quality Account 2024/25 and the outlined priorities for 2025/26, the Committee would like to express its gratitude for the thoroughness of this account. We wish to highlight the following points which were discussed during our meeting:
- Embedding a culture of Trauma Informed Care (TIC): Members welcomed the integration of trauma-informed principles into policies, procedures, practice and leadership. It was a positive that staff has reported an increased confidence and skills in engaging with people with trauma. A reduction in restrictive practice in inpatient settings suggested that the embedding had a direct effect on patient experience.
- Triangle of Care (ToC): The annual review of performance and co-production of the ToC Annual Report was completed successfully. The Trust co-designed and co-produced the care awareness training documentation which resulted in external endorsement from the Carers Trust. It was noted that training consistency was needed in the future and members welcomed the news that Carers Awareness Training would be mandated.
Based on the information provided throughout the past year, including the presentation on the draft 2024/25 Quality Account, we believe that the contents accurately represent the services provided by the Trust and align with local priorities.
Yours sincerely,
Councillor Georgina Hill
Chair, Northumberland County Council Health and Wellbeing Overview and Scrutiny Committee
Gateshead Care, Health and Wellbeing OSC
Based on Gateshead Care, Health, and Wellbeing OSC’s knowledge of the work of CNTW’s work during 2024-25 we feel able to comment as follows:
Progress Against Quality Priorities for 2024-25
OSC expressed its thanks to all staff and volunteers for the excellent work in continuing to make some real improvements in quality and safety whilst at times facing significant challenges and circumstances.
The Committee was pleased to learn that the Trust is responsive to learning opportunities on care planning from incidents that have occurred in other areas, with action plans being taken to the Board to make improvements to systems and processes.
In relation to Quality Priority 2: Delivering on key learning from key patient safety improvement themes, the OSC noted an increase in the use of restraints. It was explained that this was due to a reduction in the most severe form of restraints, with a higher occurrence of lower-level restraints being used and an increase in the recording of the use of these lower-level restraints.
Quality priorities for 2025-26
OSC is supportive of CNTW's proposed Quality Aims:
- To continue to develop and embed a positive and safe culture
- To improve physical health care
- To reduce levels of restrictive practice and violence and aggression
- To reduce levels of self harm
- To improve the care of people with a severe and enduring mental illness
Newcastle City Council
On behalf of the Health and Social Care Scrutiny Committee, I would like to thank Sarah Rushbrooke, Executive Director of Nursing, Therapies & Quality Assurance, and Lisa Strong, Deputy Director of Nursing, for attending the Health and Social Care Scrutiny Committee on Thursday 12 June 2025.
The Committee was pleased to receive the presentation provided by Sarah and Lisa and noted the following:
- There had been significant improvements across the PSIRF safety themes. The introduction of Patient Safety Learning and Improvement Panels appeared to have strengthened the framework further and the Committee would be pleased to receive feedback about the outcome of the external audit undertaken of PSIRF.
- The was an ongoing ambition to reduce the levels of restrictive practices including the elimination of prone restraint.
- The reduced incidence of the most restrictive practices combined with other new initiatives had resulted in a reduction in violence towards staff and patients.
- There had been joint working with acute health care colleagues to enable them to better look after their patients that have mental health conditions and a reciprocal arrangement to enable CNTW to better look after its patients that have physical health conditions.
- The welcome introduction of mandatory Carer Awareness training for all clinical staff.
- There had been a great deal of work undertaken to embed a culture of Trauma Informed Care. The Committee is particularly interested in this and hope that CNTW colleagues will be able to attend a meeting soon to present a more detailed account of its trauma informed practice pathway to members.
- That some of the quality aims for 2025-26 carry over important elements from the previous year, demonstrating a determination to tackle difficult issues.
During the discussion with Sarah and Lisa, the Committee heard and felt assured by the increased use of low level restrictive practices such as safety pods, instead of more risky practices such as prone restraint. The issue of restraint is a longstanding concern of the Committee and so the current direction of travel is very encouraging. The Committee also welcomed the introduction of your new model of care in the community developed at Whitehaven and which you hope will be rolled out across the North East.
I would like to extend my thanks to Sarah and Lisa for answering the Committee's wide-ranging questions and await their response to several queries they need time to investigate. I was also pleased to hear that the final version of your Quality Account would include clarification of your out of area bed figures.
Finally, the Committee hopes to continue and strengthen its relationship with the Trust. As well as the couple of points I raised earlier in my letter that we'd like to hear more about, there are some other matters that the Committee are keen to better understand. We will be in touch soon to invite Trust colleagues to one of our meetings later in the year.
Yours sincerely,
Cllr Wendy Taylor
Chair, Health and Social Care Scrutiny Committee
Healthwatch
Joint statement for the Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust's Draft Quality Account 2024/25 from the local Healthwatch in your area:
- Healthwatch Cumberland
- Healthwatch Gateshead
- Healthwatch Newcastle
- Healthwatch North Tyneside
- Healthwatch Northumberland
- Healthwatch South Tyneside
- Healthwatch Sunderland
- Healthwatch Westmorland and Furness
Thank you for sharing the draft quality account for our comment. We would like to take this opportunity to thank your team for all its hard work.
We are pleased to read about the progress with your 2024/5 priorities, particularly the work around reducing restrictive practices and embedding the triangle of care.
We continue to hear from residents that getting access to timely support and long waiting times are key issues for them and this remains a challenge.
Particularly:
- waiting for diagnosis and support from the adult neurodiversity services, particularly adult autism diagnosis and ADHD diagnoses and review pathways
- gender dysphoria service
- children and young people's services (in the areas you provide this service)
- 'bouncing between services' including crisis support, primary care support and community treatment teams.
We recognise the national challenges associated with these issues however, we are disappointed that more isn't being done to focus on what the Trust itself can do to address these issues, particularly 'bouncing between services'. We hope to see this addressed through your community transformation work.
We welcome your continued focus on improving communication with families. We hear that this continues to be a major concern with families and carers. For example, carers and service users in Sunderland have shared their experiences with us, expressing concerns about not feeling listened to or effectively communicated with. As a result, Healthwatch Sunderland is working with your involvement team to participate in several service user carer groups over the coming year, and we look forward to engaging with these groups to help develop patient-focused care.
Residents also tell us that improvements in other areas of communication are required, including:
- providing regular updates for people waiting for treatment to help manage expectations and lessen anxiety;
- improving the information provided at key points - particularly around autism diagnosis for adults, connecting people with support in their local community, including from the voluntary sector.
Local Healthwatch in rural areas continue to hear about the need for mental health support for people in the farming and agricultural communities.
We were also disappointed to read that recently published CQC inspection report (May 2025) of your wards for people with a learning disability or autism "requires immediate actions to ensure the safeguarding of people using the service" and are rated as "requiring improvement". We look forward to hearing about your improvement plans for these important services.
We also note the Integrated Care Board's decision to commission an independent review of engagement processes surrounding the closure of the Yewdale ward (inpatient facility) in Whitehaven. You will be aware that Healthwatch colleagues had heard from some local residents who felt their concerns were not being listened to.
Finally, we would like to continue to build our relationships between your different locality teams and local Healthwatch into the future.
Appendix 1
Table 18: CQC Registered Locations
|
Service Types Provided at Each Location |
Regulated Activity |
Service Type |
|||||||||
|
Treatment of disease, disorder or injury |
Assessment or medical treatment for persons detained under the Mental Health Act 1983 |
Diagnostic and Screening Procedures |
CHC |
LDC |
LTC |
MHC |
MLS |
PHS |
RHS |
SMC |
|
|
Acklam Road Hospital |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Brooke House |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Carleton Clinic |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Elm House |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Ferndene |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Hopewood Park |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Monkwearmouth Hospital |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Campus for Ageing and Vitality |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Northgate Park |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
Rose Lodge |
l |
l |
l |
|
|
l |
|
l |
|
|
|
|
Royal Victoria Infirmary |
l |
l |
l |
|
|
|
|
l |
|
|
|
|
St George’s Park |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
St Nicholas Hospital |
l |
l |
l |
l |
l |
l |
l |
l |
l |
l |
l |
|
Walkergate Park |
l |
l |
l |
|
|
l |
|
l |
|
l |
|
|
West Cumberland Hospital |
l |
l |
l |
|
|
l |
|
l |
|
|
|
Key:
CHC - Community health care services
LDC - Community based services for people with a learning disability
LTC - Long-term conditions services
MHC - Community based services for people with mental health needs
MLS - Hospital services for people with mental health needs, and/or learning disabilities, and/or problems with substance misuse.
PHS - Prison healthcare services
RHS - Rehabilitation services
SMC - Community based services for people who misuse substances.
Appendix 2
Table 19: Local Clinical Audits undertaken in 2024-25
|
National (5) |
||
|
1. |
NA-23-016.01 |
National Audit of Dementia - Spotlight Audit: Community-Based Memory Clinical Services |
|
2. |
NA-23-084.02 |
National Clinical Audit of Psychosis (NCAP) EIP Re-Audit 23-24 |
|
3. |
NA-23-080.02 |
National Audit of Inpatient Falls 23-24 |
|
4. |
NA-23-101 |
POMH-UK Topic 22a: The use of medicines with anticholinergic (antimuscarinic) properties in older people's mental health services |
|
5. |
NA-23-108 |
POMH-UK Topic 23a: Sharing Best Practice Initiatives |
|
NICE Implementation Priorities (2) |
||
|
6. |
NI-23-020.01 |
NICE (Implementation) QS95 / CG185: Psychological Therapy Use for Patients with Bipolar Disorder in a Large NHS Mental Health Trust (Adult and CYPS Services) |
|
7. |
NI-22-085 |
NICE (Implementation) QS179 Child Abuse & Neglect |
|
Trust Priorities (19) |
||
|
8. |
CA-23-105 |
CPA-PGN-06 Allocation and Reallocation of Service Users |
|
9. |
CA-23-107 |
Sexual Safety Standards |
|
10. |
CA-23-001.01 |
CPD audit for AHPs (Trust wide) |
|
11. |
CA-23-035.01 |
CYPS CPA Care and Treatment Audit |
|
12. |
CA-24-079.02 |
Medication Summaries and Discharge Letters |
|
13. |
CA-21-029 |
Re-Audit: Monitoring of Prolactin in Patients Prescribed Antipsychotic Medications and the Management of Raised Prolactin Levels in Rehabilitation Wards |
|
14. |
CA-23-027.01 |
National Audit of Inpatient Falls - Bed Rail Audit (23-24) |
|
15. |
CA-23-103.01 |
A Clinical Audit to access PURPOSE-T (Replaced Braden Scale Completion) |
|
16. |
CA-24-064.02 |
Adherence to ECTAS Standards on Time to re-orientation Post ECT |
|
17. |
CA-23-098.01 |
VTE Risk Assessment Completion audit |
|
18. |
CA-24-019.02 |
Body maps audit - Trust wide but led in North Cumbria |
|
19. |
CA-23-012.02 |
Nutrition policy audit |
|
20. |
CA-23-118 |
Trust wide Inpatient Diabetes Audit |
|
21. |
CA-24-050.01 |
Care Planning and personalisation of care planning |
|
22. |
CA-24-086.01 |
Transition of Care from CYPS to Adult Mental Health Services |
|
23. |
CA-23-091.01 |
Clinical Supervision |
|
24. |
CA-24-010.03 |
Long Term Segregation |
|
25. |
CA-23-063.02 |
Safeguarding adults at Risk |
|
26. |
CA-24-011.06 |
Seclusion Annual Audit |
|
Medicines Management Priorities (3) |
||
|
27. |
MM-22-054.01 |
Management of Acute Alcohol withdrawal in adults (PPT-PGN- 22) |
|
28. |
MM-23-053.01 |
Safe Prescribing and administration of insulin |
|
29. |
MM-23-033.01 |
The use of zuclopenthixol acetate (Accuphase) within CNTW – Re-audit (PPT-PGN- 27) |
|
CBU Priority (Community Care) (4) |
||
|
30. |
CA-22-069 |
Dental audit (North Cumbria) |
|
31. |
CA-23-071.01 |
Progress note framework |
|
32. |
CA-24-094.03 |
Clinical Audit of Unallocated Cases Awaiting Treatment. |
|
33. |
CA-24-073.01 |
Recording of supervision in clinical records |
|
CBU Priority (Inpatient Care) (3) |
||
|
34. |
CA-23-028.01 |
An audit to assess Physical Health Monitoring compliance with CNTW(C) 29 |
|
35. |
CA-23-115 |
Inpatients South CBU compliance with capacity assessments to consent to treatment in detained patients at point of admission, at 3 months, and at CTO initiation. |
|
36. |
CA-23-004.01 |
Patient Debrief Post Tertiary Intervention Joint Audit Inpatient CBU & Learning Disabilities & Autism CBU |
|
CBU Priority (Specialist Care) (1) |
||
|
37. |
CA-23-114 |
Physical health monitoring in young patients on antipsychotics in in-patient units across all inpatient CYPS wards North Cumbria |
Appendix 3
Annual Report on Safe Working Hours: Doctors in Training
1. Executive summary
This is the Annual Board report on Safe Working Hours which focuses on Resident Doctors. The process of reporting has been built into the new Resident Doctor contract and aims to allow Trusts to have an overview of working practices of Resident Doctors as well as training delivered.
All new Psychiatry Trainees and GP Trainees rotating into a Psychiatry placement are on the New 2016 Terms and Conditions of Service. There are currently 191 trainees working into CNTW on the new Terms and Conditions of Service via the accredited training scheme via NHS England. There are an additional twenty-six trainees employed directly by CNTW working as Trust Grade Doctors or Teaching/Clinical/Research Fellows.
high level data
- Number of Resident Doctors (total): 191 Trainees (December 2024)
- Number of Resident Doctors on 2016 TCS (total): 191 Trainees (December 2024)
- Amount of time available in job plan for Guardian to do the role: This is being remunerated through payment of 1 Additional Programmed Activity
- Admin support provided to the Guardian (if any): Ad Hoc by Medical Staffing Team
- Amount of job-planned time for educational supervisors: 0.5 PAs per trainee
- Trust Guardian of Safe Working: Dr Clare McLeod
2. Risks and mitigations associated with the report
- 75 Exception Reports raised during the year
- 17 fines issued
- 3 Agency Locums booked during the period covering vacant posts and sickness (this figure will differ slightly to the breakdown below as the breakdown shows locums month by month but some are in post over a few months, so this figure is the total)
- 588 shifts lasting between 4hrs and 12hrs were covered by internal doctors.
- On 14 occasions during the period the Emergency Rotas were implemented (either by emergency rota cover or by the Back-up / training rota)
- 11 IR1s submitted due to insufficient handover at admission
exception reports (regarding working hours)
|
Exception Reports Received |
||||||
|
Q1 |
Q2 |
Q3 |
Q4 |
Total Hours & Rest |
Total Education |
|
|
1 |
0 |
0 |
0 |
1 |
0 |
|
|
0 |
1 |
1 |
4 |
6 |
0 |
|
|
0 |
1 |
0 |
3 |
4 |
0 |
|
|
0 |
0 |
3 |
0 |
3 |
0 |
|
|
0 |
1 |
1 |
0 |
2 |
0 |
|
|
1 |
5 |
0 |
2 |
8 |
0 |
|
|
7 |
24 |
6 |
2 |
39 |
0 |
|
|
1 |
0 |
0 |
0 |
1 |
0 |
|
|
3 |
2 |
1 |
1 |
7 |
0 |
|
|
2 |
1 |
0 |
1 |
4 |
0 |
|
|
0 |
0 |
0 |
0 |
0 |
0 |
|
|
15 |
35 |
12 |
13 |
75 |
0 |
|
Work schedule reviews
During the year there have been 75 Exception Reports submitted from Trainees for hours and rest throughout 2024; the outcome of which was that TOIL was granted for 47 cases, payment was made on 20 occasions, no action required on 3 and 5 are yet to be responded to.
i) Locum bookings - Agency
|
Locum bookings (agency) by department |
||||
|
Specialty |
Q1 |
Q2 |
Q3 |
Q4 |
|
SGP/Northgate |
1 |
1 |
0 |
0 |
|
SNH |
0 |
0 |
0 |
0 |
|
RVI |
0 |
0 |
0 |
0 |
|
HWP |
0 |
0 |
0 |
0 |
|
MWM/GHD |
0 |
0 |
0 |
0 |
|
Cumbria |
0 |
0 |
0 |
0 |
|
Total |
1 |
1 |
0 |
0 |
|
Locum bookings (agency) by grade |
||||
|
|
Q1 |
Q2 |
Q3 |
Q4 |
|
F2 |
0 |
0 |
0 |
0 |
|
CT1-3 |
1 |
1 |
0 |
0 |
|
ST4+ |
0 |
0 |
0 |
0 |
|
Total |
1 |
1 |
0 |
0 |
|
Locum bookings (agency) by reason |
||||
|
|
Q1 |
Q2 |
Q3 |
Q4 |
|
Vacancy |
1 |
1 |
0 |
0 |
|
Sickness/other |
0 |
0 |
0 |
0 |
|
Total |
1 |
1 |
0 |
0 |
a) Locum work carried out by trainees
|
Area |
Number of shifts worked Q1 |
Number of shifts worked Q2 |
Number of shifts worked Q3 |
Number of shifts worked Q4 |
Total for Year 2023 |
|
SNH |
13 |
8 |
6 |
5 |
32 |
|
SGP/Northgate |
19 |
37 |
35 |
9 |
100 |
|
Gateshead/MWH |
15 |
61 |
32 |
6 |
114 |
|
Hopewood Park |
12 |
15 |
15 |
14 |
56 |
|
RVI |
20 |
16 |
17 |
9 |
62 |
|
CAV |
2 |
23 |
28 |
6 |
59 |
|
Cumbria |
23 |
18 |
13 |
5 |
59 |
|
North of Tyne |
16 |
12 |
20 |
13 |
61 |
|
South of Tyne |
20 |
8 |
15 |
2 |
45 |
|
CAMHs |
0 |
0 |
0 |
0 |
0 |
|
Total |
140 |
198 |
181 |
69 |
588 |
b) Vacancies
|
Vacancies by month |
|
||||
|
Area |
Grade |
Q1 |
Q2 |
Q3 |
Q4 |
|
MWM/GHD |
CT |
2 |
3 |
0 |
0 |
|
|
GP |
0 |
3 |
0 |
6 |
|
|
FY2 |
0 |
0 |
0 |
0 |
|
RVI |
CT |
1 |
0 |
0 |
0 |
|
|
GP |
3 |
0 |
0 |
0 |
|
|
FY2 |
0 |
0 |
0 |
0 |
|
SGP |
CT |
3 |
6 |
3 |
3 |
|
|
GP |
0 |
0 |
0 |
0 |
|
|
FY2 |
0 |
0 |
0 |
0 |
|
Hopewood Park |
CT |
0 |
0 |
0 |
0 |
|
|
GP |
2 |
6 |
1 |
0 |
|
|
FY2 |
0 |
0 |
2 |
0 |
|
CAV |
CT |
0 |
0 |
0 |
0 |
|
|
GP |
2 |
3 |
3 |
3 |
|
|
FY2 |
3 |
0 |
3 |
0 |
|
SNH |
CT |
2 |
3 |
3 |
3 |
|
|
GP |
0 |
0 |
0 |
0 |
|
|
FY2 |
0 |
0 |
0 |
0 |
|
Cumbria |
CT |
0 |
0 |
0 |
3 |
|
|
GP |
0 |
0 |
0 |
0 |
|
|
FY2 |
0 |
0 |
0 |
0 |
|
Total |
|
18 |
24 |
15 |
18 |
To note these training gaps have been filled by Teaching/ Research/ Clinical Fellows appointments.
c) Emergency Rota Cover
The back-up / training rota doctor can be asked to cover a gap in the standard rota to prevent the use of the emergency rota cover with the provision of alternative opportunities for this training.
|
Training Rota Cover by First on-call Trainees |
||||
|
Rota |
Q1 |
Q2 |
Q3 |
Q4 |
|
SGP |
0 |
0 |
2 0 2 0 2 0 |
0 0 0 0 0 0 |
|
SNH |
0 |
0 |
||
|
RVI |
0 |
0 |
||
|
GHD/MWM |
0 |
0 |
||
|
HWP |
1 |
0 |
||
|
NGH |
0 |
0 |
||
|
Total |
1 |
0 |
6 |
0 |
d) Fines
There were 17 fines issued during the last year due to minimum rest requirements between shifts not being met due to finishing twilight/weekend shifts late.
Issues Arising:
The numbers of Exception Reports have decreased from the 98 reported in 2023 to 75 reported in 2024.
In 2024, 47 of the Exception Reports were closed with TOIL, in 20 cases with payment, 3 no further action and 5 cases are still awaiting completion.
There were 17 fines levied in 2024, which is like the 20 the previous year, and representing an increase from previous years.
There have been 11 IR1s submitted for Insufficient Medical Handover in 2024, which is lower to the number submitted in 2023, when there were 20 IR1s for Insufficient Medical Handover.
There was a decrease in the number of times the Emergency Rota cover was used, from 21 in 2023 to 7 in 2024. The number of times the back-up / training rota was used to cover rota gaps in 2024 also fell from 30 to 7.
The number of shifts undertaken by internal doctors to cover rota gaps due to sickness, adjustments or gaps has decreased from 780 in 2023 to 588 in 2024.
Actions Taken to Resolve These Issues
Exception Reporting
The number of Exception Reports is lower than 2023 but remains higher than in previous years.
The large number of ERs from Cumbria in Q2 represents travel time between the Carlton Clinic and Whitehaven for on-call and training (as agreed by the LET to use ER for this purpose) rather than excessive workloads or a safety issue.
There were 12 ER from higher trainees in 2024, slightly reduced from 2023 when 17 were submitted by higher trainees, but the increase seen in 2023 has been maintained. The continued relative increase in exception reports from higher trainees represents a mixture of more complete reporting but also reflects the increase in workload in long day shifts and twilight shifts due to MHA work. This continues to be monitored and provisions to involve the consultant on call to take on some of the MHA work if there are more than three assessments waiting have been instigated.
Most of the Exception Reports in CNTW have been closed with Time Off in Lieu (TOIL) for 47 cases, as usual in CNTW. A proportion of the Exception Reports which had to be closed by payment was in part due to trainees having to use the Exception Reporting for travel time from West Cumbria to the Carleton Clinic where there is an agreement with the LET for remuneration rather than TOIL.
The profile of Exception Reporting continues to be raised and encouraged at induction, the Guardian of Safe Working (GoSW) forum with trainees. Screen shots of the process of completing the Exception Reporting documentation are shared at induction and via email with all trainees.
Medical Handover
The number of IR1s for Insufficient Medical Handover at admission has fallen from previous years which is encouraging. This represents a significant fall over the last 4-5 years (2023 25 IR1s; 2022 22 IR1s; 2021 46 IR1s and 2020 83 IR1s for Insufficient Medical Handover) and indicates the improvement in practice has been sustained.
Work continues in Cumbria where MHA assessments are often carried out by non-CNTW clinicians, to meet with these doctors and discuss the most appropriate means of recording and handover.
Handover between Resident Doctors has also been a focus this year with work to encourage face to face handover especially from the night shift doctor to the day team with discussion in the forum and in meetings with Resident Doctors on visits to each Trust site.
These reports continue to be reviewed and followed up by the Director of Medical Education and collated to share with staff throughout the Trust and are discussed at the GoSW forum, in addition to being shared specifically with clinical staff most involved in admissions to hospital.
The importance of medical handover both at admission and at the end of a shift will remain a priority to be discussed at induction (with instruction on how to fill in the IR1 documentation and sharing of screen shots of the process by email) and in the forums mentioned and continue to be monitored accordingly.
Emergency Rotas
There has been further decreases in the use of the Emergency Cover Rota and the Back- up / training rota in 2024. These arrangements are necessary if there is a rota gap which, despite the efforts of Medical Staffing, is not filled by 3pm. The use of these rotas is discussed at the GoSW forum with monitoring procedures in place to ensure there is no compromise to safety. It can be a concern to trainees with the need to work in less familiar sites, the increased geographical area to cover and the potential increase in workload in the case of rota collapse. Video inductions for each of the Trust sites are kept updated and doctors are encouraged to watch these videos prior to commencing a shift if they are not familiar with the site as well as linking in with the doctor handing over for any other queries about the site.
The training rota was introduced in August 2020, primarily to provide core and GP trainees the opportunity to shadow the Higher trainees to gain experience in emergency psychiatry and Mental Health Act Assessments. It also serves to cover vacant shifts with the Resident Doctor on the training rota moving to cover a gap and therefore preventing the need to implement the Emergency Cover Rota. It is encouraging that the reductions in need for this rota have been sustained and therefore the training offered with this rota has been in the main been provided.
The reduction in use of the emergency and back-up / training rotas is encouraging as is the reduction in the number of locum shifts covered by resident doctors. This is mainly due to the changes in the allocation of teaching fellows out of hours provision and a new innovative clinical fellow post covering rota gaps.
Fines
There were 17 fines issued in 2024 due to breaches of the length of shifts, the minimum rest periods between resident on-call shifts or during non-resident on-call shifts, which is like the number levied in 2023. These fines were spread across both higher and core training rotas and across all rotas in the Trust. The increase in breaches of shift length and rest in higher training rotas relates to mainly to work intensity on twilight shifts and long day shifts due to MHA assessment but also represents more complete reporting from higher trainees which is encouraging.
It was agreed at the GoSW forum to spend the fine money on non-perishable food and drinks for on-call and mess rooms, with the money divided out by the number of trainees at each site. Money is spent to the benefit of all trainees and as timely as possible so that the current trainees benefit.
Mess Rooms
Over this year, there have been discussions about the re-provision of mess room facilities for Resident Doctors in all the Trusts in the region. St George’s Park has had a mess room for some time which is much valued and used daily. Therefore, discussions have focused on a similar provision at all our sites which has largely been successful. The mess room at St Nicholas Hospital had been in Hartside, but this room was too small for the numbers of trainees especially with the relocation of services from CAV in 2025, so there are now discussions with Estates about sourcing a room in the Bamburgh Clinic. There are on-going discussions with estates about options for Hopewood Park.
Resident Doctors Forum
The forum returned to a hybrid in person / teams meeting in March 2022. Over subsequent meetings the numbers attending in person have gradually increased with the majority now in person. We will continue the hybrid model which was in place before the pandemic to allow people to attend without the need to travel.
Summary
The number of Exception Reports has decreased in 2024 in comparison to 2023 but remains higher than previous years with the majority closed through TOIL. Work will continue to increase the level of completeness of reporting.
It is encouraging to see the fall in the number of reports of Insufficient Medical Handover being sustained which will continue to be encouraged and the completeness of handover promoted in a variety of forums.
There has been a fall in the number of occasions where the Emergency Cover rota and Back-up /training rota were necessary, which is encouraging. This will continue to be monitored.
The Resident Doctor’s Forum is well attended and will continue using a hybrid model to allow both in person and remote attendance.
Dr Clare McLeod
Guardian of Safe Working for CNTW
Dr Rajesh Nadkarni
Executive Medical Director
December 2024
Appendix 4
Statement of Directors' Responsibilities in respect of the Quality Report
The directors are required under the Health Act 2009 and the National Health Service (Quality Accounts) Regulations to prepare Quality Accounts for each financial year.
NHS Improvement has issued guidance to NHS foundation Trust boards on the form and content of annual quality reports (which incorporate the above legal requirements) and on the arrangements that NHS foundation Trust boards should put in place to support the data quality for the preparation of the quality report.
In preparing the quality report, directors are required to take steps to satisfy themselves that:
- the content of the quality report meets the requirements set out in the NHS foundation Trust annual reporting manual 2024-25 and supporting guidance Detailed requirements for quality reports 2024-25
- the content of the quality report is not inconsistent with internal and external sources of information including:
- board minutes and papers for the period April 2024 to May 2025
- papers relating to quality reported to the board over the period April 2024 to May 2025
- feedback from commissioners
- feedback from governors
- feedback from local Healthwatch organisations
- feedback from overview and scrutiny committee
- the Trust’s Annual review of complaints information which was presented to the Board within the Safer Care (Quarter 4) report published under Regulation 18 of the Local Authority Social Services and NHS Complaints Regulations 2009
- the 2024 national patient survey
- the 2024 national staff survey
- the Head of Internal Audit’s annual opinion of the Trust’s control environment dated
- CQC inspection report dated 04/08/2022
- the quality report presents a balanced picture of the NHS foundation Trust’s performance over the period covered.
- the performance information reported in the quality report is reliable and accurate.
- there are proper internal controls over the collection and reporting of the measures of performance included in the quality report, and these controls are subject to review to confirm that they are working effectively in practice.
- the data underpinning the measures of performance reported in the quality report is robust and reliable, conforms to specified data quality standards and prescribed definitions, is subject to appropriate scrutiny and review.
- the quality report has been prepared in accordance with NHS Improvement’s annual reporting manual and supporting guidance (which incorporates the quality accounts regulations) as well as the standards to support data quality for the preparation of the quality report.
The directors confirm to the best of their knowledge and belief they have complied with the above requirements in preparing the quality report.
By order of the Board
Darren Best, Chair
James Duncan, Chief Executive
Appendix 5
Limited Assurance Report on the content of the Quality Account
Information not required to be included within the Quality Account 2024-25 as per direction from NHS Improvement.
Assurance work on quality accounts and quality reports should cease, and no limited assurance opinions are expected to be issued in 2024-25. Where auditors have completed interim work or early testing on indicators, auditors should consider whether value can be derived from work already completed, such as a narrative report being provided to the Trust, or governors at an NHS foundation Trust. For NHS foundation Trusts, there is no formal requirement for a limited assurance opinion or governors’ report.
Appendix 6
Glossary
A&E - Accident & Emergency department.
ADHD - Attention Deficit Hyperactivity Disorder – a group of behavioural symptoms that include inattentiveness, hyperactivity and impulsiveness.
AIMS - Accreditation for Inpatient Mental Health Services.
ASD - Autism Spectrum Disorder.
Bed days - The number of days that a hospital bed is occupied overnight.
Blanket restriction - Rules or policies that restrict a service user’s liberty and other rights, which are routinely applied to a group of service users without individual risk assessments to justify their application.
CAMHS - Children and Adolescent Mental Health Services. In CNTW we usually refer to our services as CYPS (see below).
Casemix - a term used to identify groups of statistically similar patients.
CCG - Clinical Commissioning Group – a type of NHS organisation that commissions primary, community and secondary care from providers.
CAS alert - The Central Alerting System is a web-based cascading system for issuing patient safety alerts, important public health messages and other safety critical information and guidance to the NHS.
CCQI - College Centre for Quality Improvement – part of the Royal College of Psychiatrists, working with services to assess and increase the quality of care they provide.
CGI - Clinical Global Impression Rating Scale.
CNTW - Cumbria, Northumberland, Tyne and Wear NHS Foundation Trust.
Commissioner - Members of Clinical Commissioning Groups (CCGs), regional and national commissioning groups responsible for purchasing health and social care services from NHS Trusts.
CQUIN - Commissioning for Quality and Innovation – a scheme whereby part of our income is dependent upon improving quality.
Clinician - A healthcare professional working directly with service users. Clinicians come from several healthcare professions such as psychiatrists, psychologists, nurses and occupational therapists.
Cluster/ clustering - Mental health clusters are used to describe groups of service users with similar types of characteristics.
CQC - Care Quality Commission – the independent regulator of health and adult social care in England. The CQC registers (licenses) providers of care services if they meet essential standards of quality and safety and monitor them to make sure they continue to meet those standards.
CPA - Care Programme Approach – a package of care for some service users, including a care coordinator and a care plan.
CRIS - Clinical Record Interactive System allows researchers to conduct research using the large amount of information from electronic patient records.
CTO - Community Treatment Order.
CYPS - Children and Young Peoples Services – also known as CAMHS.
Dashboard - An electronic system that presents relevant information to staff, service users and the public.
DOLS - Deprivation of Liberty Safeguards – a set of rules within the Mental Capacity Act for where service users cannot make decisions about how they are cared for.
Dual Diagnosis - Service users who have a mental health need combined with alcohol or drug usage.
ECT - Electroconvulsive therapy.
EIP - Early Intervention in Psychosis.
Forensic - Forensic teams provide services to service users who have committed serious offences or who may be at risk of doing so.
Freedom to Speak Up - Encouraging and supporting staff to raise concerns at work, based on recommendation from Sir Robert Francis’ Freedom to Speak Up Review in response to the Mid-Staffordshire scandal.
Friends and Family Test (FFT) - A process for people who use NHS services to provide feedback on their experience.
FTE - Full-Time Equivalent, a unit of employment that accounts for some people working part-time.
Gatekept - Gatekeeping involves assessing the service user before admission to hospital to consider whether there are alternatives to admission.
GP - General Practitioner – a primary care doctor.
HDAT - High Dose Antipsychotic Therapy.
HQIP - The Healthcare Quality Improvement Partnership promotes quality in healthcare, and to increase the impact that clinical audit has on healthcare quality improvement.
IAPT - Improving Access to Psychological Therapies – a national programme to implement National Institute for Health and Clinical Excellence (NICE) guidelines for people suffering from depression and anxiety disorders.
Integrated Care Board (ICB) - A statutory NHS organisation responsible for developing a plan for meeting the health needs of the population, managing the NHS budget and arranging for the provision of health services in the Integrated Care System (ICS) area.
ICD10 - International Classification of Diseases (ICD) 10th Revision, used to code diagnoses.
Injection Rapid Tranquilisation - Injection rapid tranquilization is given when people are very distressed and are unable to accept oral rapid tranquilization medication.
Integrated Care System (ICS) - A collaborative arrangement where NHS organisations, local councils and others take collective responsibility for managing resources, delivering NHS standards, and improving the health of the population they serve.
LD - Learning Disabilities.
LeDeR - The Learning Disabilities Mortality Review Programme aims to make improvements in the quality of health and social care for people with learning disabilities, and to reduce premature deaths in this population.
Lester Tool - The Lester Positive Cardiometabolic Health Resource provides a simple framework for identifying and treating cardiovascular and type 2 diabetes risks in service users with psychosis receiving antipsychotic medication.
LGBT - Lesbian, Gay, Bisexual, and Transgender.
MHCT - Mental Health Clustering Tool – a computerised system used in clustering.
Mechanical Restrain Equipment (MRE) - Mechanical Restrain Equipment. Mechanical restraint is the use of a device such as metal or soft cuffs and/or belts to prevent or restrict movement of a person’s body or part of the body and should only be considered as a last resort.
Multimorbidity - Relating to service users with several co-occurring diseases.
NHS - National Health Service – the publicly funded national healthcare system for England
NHS England/ Improvement - The independent regulator of NHS Foundation Trusts, ensuring they are well led and financially robust.
NEQOS - North East Quality Observatory System – an organisation that helps NHS Trusts to improve quality through data measurement.
NICE - National Institute for Health and Care Excellence – an organisation that produces best practice guidance for clinicians.
NIHR - National Institute of Health Research – an NHS organisation undertaking healthcare related research.
NRLS - National Reporting and Learning System – a system for recording patient safety incidents, operated by NHS Improvement.
OPS - Older Peoples Services.
Oral Rapid Tranquilisation - Oral rapid tranquilization is a medication that can be offered or can be requested if a person is struggling with distress and other non-medication options have not reduced the person’s distress.
Out of area placements - Service users admitted inappropriately to an inpatient unit that does not usually receive admissions of people living in the catchment of the person’s local community mental health team.
Pathway - A service user journey through the Trust, people may come into contact with many different services.
Personality Disorder - a class of mental disorders characterized by enduring maladaptive patterns of behaviour, cognition, and inner experience.
PHSO - The Parliamentary and Health Service Ombudsman.
PICU - Psychiatric Intensive Care Unit.
POMH-UK - Prescribing Observatory for Mental Health – a national organisation that helps mental health Trusts to improve their prescribing practice.
PMVA - Prevention and Management of Violence and Aggression
Prone Restraint - Prone restraint is when the person being restraint will be held chest down, some people find this type of restraint more traumatic than other forms.
QPR - Process of Recovery Questionnaire, a patient reported outcome measure.
Rapid tranquilisation - When medicines are given to a person who is very agitated or displaying aggressive behaviour to help quickly calm them.
REACT - Relatives Education and Coping Toolkit, an online self-help package for relatives and friends of people with mental health problems
Recovery College - Recovery Colleges take an educational approach to provide a safe space where people can connect, gain knowledge and develop skills.
Restraint - Restraint is any direct physical contact, or application of force, by staff towards patients where the intention is to prevent, restrict or subdue movement. This could range from Guiding a confused patient to floor based restraint.
RiO - CNTW’s electronic patient record
RTT - Referral to Treatment – used in many waiting times calculations
Seclusion - Seclusion is a specially designed low stimulus room with not many items in it, people are supported in seclusion for the shortest time possible. Seclusion is only for when people are extremely distressed.
Serious Incident - An incident resulting in death, serious injury or harm to service users, staff or the public, significant loss or damage to property or the environment, or otherwise likely to be of significant public concern. This includes ‘near misses’ or low impact incidents which have the potential to cause serious harm.
Single Oversight Framework - An NHS Improvement framework for assessing the performance of NHS Foundation Trusts (replacing the Monitor Risk Assessment Framework)
Talk 1st - Part of CNTW's Positive & Safe Care Strategy. We aim to reduce violence and aggression, and restrictive interventions.
Transition - When a service user moves from one service to another, for example from an inpatient unit to being cared for at home by a community team.
Triangle of Care - a national scheme, to promote therapeutic alliance between the service user, their mental health professional and their carers.
Tyne and Wear Citizens Programme - The local chapter of Citizens UK, organising communities to act together for power, social justice and the common good.
VA - Violence and Aggression.
Your Voice - An CNTW service user and carer feedback system that allows us to evaluate the quality of services provided
For other versions telephone 0191 246 6935 or email qualityassurance@CNTW.nhs.uk
Copies of this Quality Account can be obtained from our website (www.cntw.nhs.uk) and the NHS Website (www.nhs.uk).
If you have any feedback or suggestions on how we could improve our Quality Account, please do let us know by emailing qualityassurance@CNTW.nhs.uk or calling 0191 246 6935.
Printed copies can be obtained by contacting:
Commissioning and Quality Assurance Department St Nicholas Hospital
Jubilee Road, Gosforth Newcastle upon Tyne NE3 3XT
Tel: 0191 246 6935