Physical and Public Health Strategy 2025 - 2028
National context
In July 2025 "Fit for the Future" 10-Year Health Plan was published by the government, aiming to modernise the NHS through three main shifts: moving care from hospitals to communities, from treatment to prevention, and transitioning from analogue to digital.
A few months later, NHSE produced the Medium Term Planning Framework for the NHS. The framework sets out the priority deliverables and the reform opportunities that Integrated Care Boards and providers need to deliver for the next 3 years and the broader strategic aims that will need to be reflected in 5-year plans developed by each organisation.
The framework is supported by a financial framework to allow organisations to move from annual short-term planning to 3-year plans for investment and savings in order to restore financial discipline across the NHS.
For mental health and learning disabilities the medium-term planning framework sets out the following commitments which align to service changes we have committed to as part of this planning framework.
- Continue to expand coverage of mental health support teams in schools and colleges ahead of the ask for full national coverage by 2029
- develop a plan for delivering their local approach to establishing mental health emergency departments co-located with or close to at least half of Type 1 emergency departments by 2029
- use ring-fenced funding to support the delivery of effective courses of treatment within NHS Talking Therapies and reduce ill-health related inactivity through access to Individual Placement and Support for people with severe mental illness
- reduce inappropriate out-of-area placements and locked rehabilitation inpatient services. From 2027/28 onwards, ICBs should only commission mental health inpatient services for adults and older adults that align with the NHS Commissioning Framework
- reduce longest waits for CYP community mental health services by improving productivity, and reducing local inequalities and unwarranted variation in access
- identify and act on productivity opportunities including, in children and young people’s community mental health services, increasing the number of direct and indirect contacts per whole time equivalent hours worked, and reducing the average length of stay in adult acute mental health beds
- ensure mental health practitioners across all providers undertake training and deliver care in line with the Staying safe from suicide guidance, which sets out the latest evidence in understanding and managing suicide
- reduce the very longest lengths of stay in mental health hospitals for people with learning disability and or autism
- reduce admission rates to mental health hospitals for people with a learning disability and autistic people
- optimise existing resources to reduce long waits for autism and ADHD assessments and improve the quality of assessments by implementing existing and new guidance, as published
In 2023, CNTW launched its strategy for the future to work together, with compassion and care, to keep you well over the whole of your life. The strategy sets out five strategic ambitions to deliver the goals and changes we want to see across our services both now and in the future.
We recognise the need to deliver better, easier access to care and support for the people and communities that we serve, in partnership with others, and the need to ensure that our specialist clinicians can offer effective, evidence-based care and support. The current way our services and the system we work in is set up does not enable us to do this consistently.
We have a good track record on delivering quality, safe services, and generally our services perform comparatively well. However, we recognise that there are significant waits to access some of our services, real pressures on getting urgent and crisis support at times, and a lack of consistency in how we deliver services well across all the communities that we serve.
We also recognise that the Care Quality Commission has identified areas for us to improve, and we are focussed on embedding these improvements. The CQC has recognised that we have a clear and ambitious strategy, and that we work as a good partner. They have also found that we need to make improvements to our governance (the way the systems within the organisation work) and ensure that our people feel consistently valued, supported and well led. We now want to set out clearly our direction for improvement of our services so that we can engage our public, our people and our partners early and effectively in designing and delivering that change.
We have a good track record on delivering our financial goals, but, like most NHS organisations we face real challenges in recovering an underlying financial gap that has developed through the last five years. Our three year plan commits us to delivering long term sustainability, while ensuring we match income and expenditure each year. We have built our expectations on financial delivery into our proposals for service change, and expect all of the changes we propose to be funded within the resources that are available to us over the next three years.
Our strategy and Model of Care and Support is fully aligned to the NHS 10-year plan and the commitments in here for services for people with mental health needs, and people with a learning disability, neurodivergence or neurological disorders.
We are ambitious and focussed on delivering on the aspirations of the ten year plan through our strategy. We set out here the key service changes that we want to make to deliver better services over this and the next two years, living within our means and creating a better more joined up and consistent offer for the people and communities we serve.
Addressing health inequalities
Tackling health inequalities is a key priority for this plan. We know that people’s mental health and wellbeing are affected by where they live, their income, housing, employment, physical health, and access to support.
Across the communities we serve, some people experience poorer mental health, longer waits for care, and more barriers to getting help. This plan aims to close these gaps by bringing services closer to neighbourhoods, improving early access to support, and making sure care is fair and consistent across all areas.
By working closely with local partners, including GPs, councils, voluntary organisations and community groups, we will focus our resources where need is greatest, support people earlier, and reduce avoidable hospital admissions. These changes are designed to help ensure everyone has a better chance of getting the right support at the right time, regardless of where they live or their circumstances.
Summary of the proposed strategic plans
In line with our strategic objectives and model of care and support, CNTW is undertaking a series of service developments across community, inpatient, crisis, learning disability, neurodevelopmental and specialist pathways. Although each scheme focuses on different services, they are driven by the same challenges: rising demand, increasing complexity, workforce pressures, buildings that are no longer suited to modern models of care, and long waits or bottlenecks that prevent people from moving smoothly through the system. Addressing these issues together, rather than in isolation, will create a more joined up and sustainable approach to the services we provide across the North East and North Cumbria.
Across the Trust, several core areas are being taken forward. These include:
- Improving access to community mental health care, with neighbourhood mental health centres, better triage, and more personalised support.
- Strengthening urgent care, including mental health emergency departments, access to crisis assessment and treatment services modernised s136 suites.
- Reviewing acute inpatient staffing models, including enhanced MDT working and seven day senior decision making.
- Updating rehabilitation pathways, ensuring inpatient beds meet national standards and strengthening community based recovery options.
- Redesigning and reconfiguring older adult inpatient services to reduce delays and create modern, fit for purpose wards.
- Re-shaping learning disability inpatient care, consolidating beds and expanding the Learning Disability In Reach and Transition Team.
- Improving ADHD and Autism pathways, including a region wide re triage to reduce waits.
- Modernising secure services and the Northgate site, with clearer pathways, reduced out of area placements and better use of estate.
- Reviewing children and young people’s inpatient capacity, aligning beds to need and strengthening community alternatives.
- Transforming adult eating disorder services, shifting to more community based intensive support.
Viewing these developments together allows us to coordinate decisions, avoid duplication, share resources, and ensure each change supports the wider system. People will experience more coordinated care, more support closer to home, fewer unnecessary hospital stays, and clearer, more consistent pathways across the region. Changes will be phased, with full engagement and support. Some teams may work differently or in new locations, but the focus is on building sustainable, safer and more resilient services.
Wider benefits will include:
- More care delivered in communities, reducing pressure on inpatient units.
- Faster access to evidence based treatments.
- Safer and more modern inpatient wards where they are needed.
- Reduced out of area placements.
- A more consistent model of care across localities.
- Better use of buildings, staffing and resources.
- A more stable and sustainable system for the future
A major area of change is improving access to support in communities. Work is underway to strengthen Community Mental Health Teams through clearer referral routes, faster triage, more personalised care planning and better involvement of carers. Neighbourhood mental health centres, such as Hope Haven, are being developed to offer walk in support, short stay beds and links to wider services such as housing and employment. These hubs aim to provide earlier intervention and reduce the need for hospital admission, while improved coordination with GPs, social care and voluntary sector partners ensures people receive more holistic and preventative support.
At the same time, urgent and crisis care is being modernised to provide safer and more appropriate environments. This includes redesigning Section 136 places of safety, developing Mental Health Emergency Departments, and expanding crisis alternatives like safe havens. These improvements will help reduce pressure on A&E and crisis teams and ensure people in crisis receive timely and expert assessment in the right setting.
The Trust is also reviewing acute inpatient staffing models to ensure wards remain safe and effective, including the introduction of an enhanced multi disciplinary team approach and routine seven day senior clinical decision-making.
Alongside this, broader inpatient pathways are being strengthened. Rehabilitation services are being reviewed, including proposals to refurbish Willow View and reconsider the function of Elm House, creating a more coherent community to inpatient recovery pathway. Older adult inpatient services need to be redesigned to reduce long delays for people who are medically ready to leave hospital, exploring options such as consolidating wards, step up/step down care and new community partnerships.
Learning disability services are also evolving. Low inpatient occupancy and operational challenges at Rose Lodge led to the temporary consolidation of specialist beds at Edenwood, supported by a new Learning Disability In Reach and Transition Team. This team now supports people with learning disabilities on general mental health wards, offering assessments, communication support and discharge planning. Longer term decisions about bed locations and future models will be informed by engagement with service users, carers, staff and partners.
A region wide redesign of ADHD and autism assessment pathways is underway to make waiting times fairer and more consistent. This includes introducing a clearer triage approach and ensuring people are directed to the most appropriate type of support across NHS services, local councils, and voluntary and community organisations.
We are also progressing improvements to secure services and the Northgate site, reducing the need for people to receive care outside the region and strengthening specialist pathways. Alongside this, a full review of children and young people’s inpatient capacity is taking place to ensure services reflect changing levels of need and complexity. Adult eating disorder services are also being modernised, with a greater emphasis on community based care rather than reliance on hospital admission.
Delivering these schemes together ensures that improvements in one part of the system support improvements elsewhere. Stronger community services reduce inpatient pressure; modern crisis pathways ease emergency demand; and clearer specialist pathways help people move through care more smoothly. Taking a whole system approach allows CNTW to make better use of staff, buildings and resources resulting in safer, more consistent and more accessible care for the future.
It is important to state that this service change plan does not cover all of the services across the CNTW footprint and will be reviewed and updated on an annual basis in line with our medium term planning framework. This plan focussing on those areas which we will be prioritising for change and improvement during 2026/27.
This service change plan will be used to underpin our single engagement narrative for internal and external use to describe the Trusts plans for service change over the coming 12 – 24 months. We want this page to set out our key areas of change which we will be informing you of and engaging you in as part of taking these plans forward.
We have prepared this in order to provide:
- A single ‘story’ for our plans for change across a range of our services. This will enable a fuller understanding for staff to describe why, how, when and with whom. It will allow for early communication and involvement of service change plans including the link to our workforce planning.
- A single ‘story’ for our plans for change across a range of our services to help public, patient and carer understanding of the whole picture of mental health and disability services. This will enable early communication and involvement of service change (helping us to identify key stakeholders early on, as well as allowing us to describe the desired impact and outcomes for patients, carers and the public.
- A single ‘story’ for our plans for change across a range of our services to help wider partners and key stakeholders, understand of our direction of travel for mental health and disability services. This will also enable us to engage with key stakeholders including Local Authority Health Overview and Scrutiny Committees and Health and Wellbeing Boards early in terms of communication, engagement and involvement. It will also allow us to plan better with key partners i.e., commissioners, in terms of governance processes and decision-making.
This service change plan will not remove, or replace, the need for individual engagement and consultation exercises for each specific service change, however it is informing our partners, public and staff of the areas of change and development we have planned.
Difference between engagement and consultation
It is important to distinguish between the role and responsibilities for engagement, consultation and decision-making relating to service change.
While there is no legal definition of what constitutes service change, it broadly encompasses any change to NHS services which involves a shift in the way front line health services are delivered, usually involving a change to the range of services available and/or the geographical location from which services are delivered.
Engagement
NHS Trusts and Foundation Trusts, as Providers of services, have a duty to make arrangements for the engagement with, and involvement of, stakeholders (including patients, carers and the public) in the planning or provision of services.
Engagement helps to develop relationships with stakeholders who have links to health and care. It provides an opportunity to share strategic ambitions, proposals for service change (at the development stage – before options are decided), the rationale for change, and more importantly, to seek the views of others to inform any proposals or future decisions. It is a two-way process which gives people an opportunity to contribute to the development of options and service delivery.
It is important that we engage thoroughly, before any formal consultation need is considered and to establish whether any further options to initial proposals have been, or could be, considered. This stage of engagement is known as ‘pre- engagement’.
Consultation
Consultation is a formal process used in service change and has some statutory, and legal requirements. Whether formal consultation is required is determined at the strategic business case stage (submitted by the Provider to the commissioner of services) outlining the proposals for the case for service change.
The decision to enter a formal consultation stage is taken by the Commissioners (i.e., NENC ICB) and will involve discussion with NHS England. Where pre-engagement is undertaken by Providers, if formal consultation is required, this is undertaken, and led by, the Commissioners (with support from the Provider organisation). In making the decision to formally consult, commissioners will consider the following:
- Are services being completely withdrawn.
- Are services moving to another location which could cause ‘considerable disruption’ for service users.
- Will a particular cohort be unfairly disadvantaged by the proposals.
- Consideration of the level of engagement activity already undertaken by the Provider.
- The level of engagement already undertaken by the Provider with organisations including Healthwatch, Local Authority Health Overview and Scrutiny Committees and others.
Single engagement narrative – benefit
The advantage of a single engagement narrative outlining each individual service change planned will create a ‘story of the whole’ to underpin ‘the sum of its parts’. This will create a ‘no surprise’ approach to all stakeholders involved in, or who has a stake in, the Trust and its business.
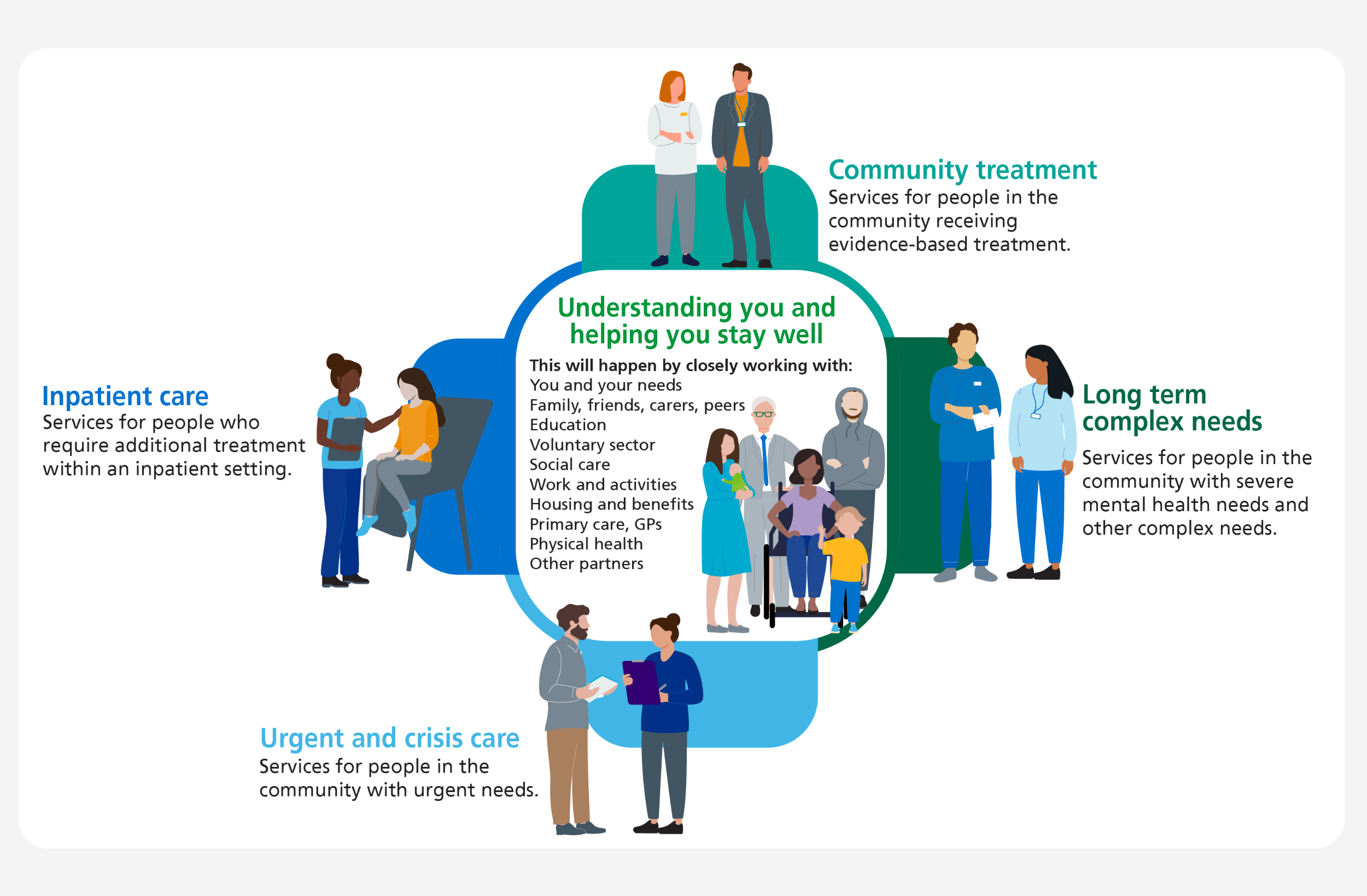
Following the release of the 10-year plan in 2024/2025, we have built on the commitments and ambitions set out in our strategy to develop our model of care and support, which will be rooted in the integration and collaboration with partners at a neighbourhood level to really understand the needs of people and support them to stay well.
This model will enable the delivery of our ambitious plan by communities and organisations working together to reduce repeated referrals, meet people’s needs earlier, and help them stay well. By drawing on individual and community strengths and removing service boundaries, support can be tailored and preventative, improving mental health, wellbeing, and active citizenship.
Some individuals will still require secondary care, which can be accessed when needed. The Trust will partner in prevention and lead on secondary care, but community support remains essential throughout. We will be developing more 24/7 Neighbourhood Mental Health Centres, similar to our successful national pilot in West Cumbria.
We will also develop Mental Health Emergency Departments to support patients to avoid attending or being admitted to hospital. This focus will reduce the demand across all our services by supporting peoples wider unmet need and helping them to stay well and avoid becoming unwell and preventing hospital admission.
Our strategic plans also include rolling out digital enabled care that improves patient experience and our productivity. These innovations include patients accessing our electronic patient record system through a portal and further rolling out of our innovation-leading single care record system for multiple partners that will mean better joined up care between organisations between partners.

To improve how our Community Mental Health Teams (CMHTs) work and to bring care closer to neighbourhoods, we are making a number of important changes. These changes support the national Personalised Care Framework and the national Community Mental Health Transformation programme, which aim to ensure that people receive care that is more flexible, more personal, and better connected to their local community.
The changes we aiming to make are as follows:
Improving access to CMHT services:
This involves reviewing how people are referred, how quickly they are seen, and how we support those who may disengage from services. Early improvements include clearer referral criteria and better communication with referrers, including how we integrated with services across our communities to improve easier access to mental health support. Making care more personalised and recovery focused
This includes updating care plan templates, promoting co production with service users, and training staff so that every care plan reflects the person’s goals, strengths and needs. Regular audits help ensure quality and consistency.
Making care more personalised and recovery focused:
This includes updating care plan templates, promoting co production with service users, and training staff so that every care plan reflects the person’s goals, strengths and needs. Regular audits help ensure quality and consistency.
Strengthening links with community partners:
We are working more closely with GPs, social care, and voluntary and community sector organisations (VCSE) so that people can access a wider range of support locally, not just within specialist mental health services.
Expanding access to evidence based interventions:
This includes improving access to psychological therapies, using outcome measures more consistently, and supporting staff to deliver interventions that are proven to help people in their recovery.
Together, these changes will make it easier for people to get the right support, improve the quality and consistency of care, and strengthen the connections between mental health services and local communities.
Easier to access to services in our communities
Community Mental Health Teams (CMHTs) play an essential role in making sure people can access the right support at the right time, close to home. We are improving how these teams work so that care is more flexible, personal and responsive to individual needs.
We are offering appointments and advice in a wider range of community locations, including CMHT bases and new spaces such as Hope Haven in Whitehaven. When needed, staff also provide home visits to people who may find it difficult to attend appointments because of their mental health, mobility issues, anxiety or social circumstances. For example, home visits are often arranged for people experiencing a relapse in psychosis, helping staff intervene early and reduce the risk of hospital admission. Telephone and video appointments are also available to make accessing support easier and more convenient.
We have introduced a new waiting times approach so that referrals are reviewed quickly and consistently. Every referral is triaged to understand the person’s level of need and any immediate risks. Once allocated, people are offered an initial assessment where staff explore their mental health, strengths, challenges and goals. This allows urgent situations such as a sudden deterioration in mental health, to be identified early so support can begin quickly, which may include a medication review, increased contact or psychological therapy.
We are strengthening personalised care planning so that each person has a clear, meaningful plan tailored to their needs. Plans include early warning signs, what to do if symptoms worsen, and how to get help in a crisis.
We are improving how we involve and support carers, recognising the vital role they play in a person’s recovery and wellbeing. Staff now routinely ask whether someone has a carer and record this in their notes so carers can be appropriately included. Carers’ knowledge and experience are valued, and they are treated as partners in care while the individual’s rights to privacy and consent are respected. Carers are also invited to contribute to service improvements and share ideas for how support can be strengthened.
Joining up how we work with partners
CNTW is working with local partners to bring mental health support closer to where people live.
As part of the national NHS 10-year Plan, we are developing neighbourhood mental health centres (NMHCs), welcoming spaces in the community where people can get help and advice without needing to go through hospital services. These hubs offer walk in support, short stay respite beds and links to practical help such as housing, employment and wellbeing services. The aim is to make it easier for people to find the right support early, in a place that feels approachable and familiar.
Hope Haven in Whitehaven is one of the new neighbourhood mental health centres. It provides a friendly, judgement free space for adults in Copeland to talk about their mental health, get emotional support and access help with practical challenges. People can walk in without a GP referral and speak to trained staff about anything affecting their wellbeing. Hope Haven brings together NHS staff and community organisations to offer a wide range of help, including:
- Drop in support for emotional wellbeing and mental health
- One to one listening and guidance
- Help with housing, employment, finances and other practical issues
- Connections to local health, social care and voluntary support
- A “Virtual Safe Haven” offering online appointments
- Short stay flats that provide calm, supportive respite outside of hospital
The Trust are hoping to expand the provision of these neighbourhood mental health centres into Carlisle, Northumberland, Newcastle and Sunderland as part of the latest round of capital applications for funding from NHSE. Community Mental Health Teams will work closely with these hubs and a wide network of partners to make sure people receive joined up support.
Staff regularly link with GPs to ensure safe, consistent care, including sharing medication advice. They also help people access wider community resources such as peer support groups, recovery colleges, employment programmes and social activities. This joined up approach ensures people receive holistic, personalised support that meets their mental, physical and social needs.
Quicker access to evidence-based treatments
Across England, more people are seeking help for their mental health, which has led to increasing pressure on Community Mental Health Teams (CMHTs). As a result, many people still wait several weeks for follow up appointments, with typical waits of around six to seven weeks in many areas.
Neighbourhood mental health hubs, such as Hope Haven, are being developed to help reduce these pressures by offering early, walk in support without the need for a referral. These hubs act as an easier “front door” to mental health care, helping people get advice, reassurance and practical help much sooner than traditional referral routes.
A number of new approaches are being introduced nationally to improve access to proven, effective mental health support. Community hubs offer immediate help and can guide people towards more formal CMHT care when needed, helping to ease waiting lists. Online therapy, regular check ins and early triage also allow people to receive guidance and coping strategies while they wait for longer term treatment.
There is also a strong focus on recovery based support. This includes help with early warning signs of relapse, practical problem solving and building confidence in managing day to day challenges. These approaches complement clinical treatments and help people stay well for longer.
Services are also looking at how CMHTs, crisis teams and community hubs can work more closely together as part of a joined up system. This more coordinated approach aims to ensure that people who need urgent help are identified quickly, support can be stepped up without delay and everyone has fair access to safe, effective care.
These developments are designed to help people receive mental health support earlier, more easily and in a way that meets their needs in the heart of their community.
We know that changing how our community teams work and what we offer will be a significant part of managing these changes well across the significant geography we offer and where we need to prioritise clinical skills and resource to meet the needs of local populations. This will include changing historical commissioning arrangements to ensure we use our resources in the areas of greatest need.
Intensive and assertive management of people with severe and enduring mental illness
What the service is and who it helps:
The Trust provides care and treatment for people living with severe and long term mental health difficulties across the North East and Cumbria. Because our organisation covers such a wide area, we deliver support in a range of settings, including inpatient services, urgent care, community treatment teams, physical health monitoring and long term recovery and support.
Our aim is to help people whose mental health conditions have a significant impact on daily life and may present a risk to themselves or others.
Community Treatment Teams currently provide a broad range of evidence based interventions. These include psychiatric and psychological treatment, mental health nursing, physical health monitoring, social work support, occupational therapy and peer support.
Support for people with the most complex needs particularly those who found it difficult to stay engaged with mainstream services are currently provided in general community teams not as a specific service.
Why change is needed:
Following the tragic events in Nottingham in June 2023 involving Valdo Calocane, NHS England requested urgent assurance from all mental health trusts about how patients with Assertive and Intensive care needs are being supported.
CNTW has carried out substantial work to identify, review and monitor people who fall into this category. By mapping this group across localities, we now understand how many patients meet specific clinical and risk criteria and what workforce capacity is needed to support them safely.
This work has made it clear that demand and resourcing do not currently match. Some areas have significantly more staff than others despite having similar levels of need. To provide safe and effective care, we will need to move resources across localities.
NHS England has so far not identified new funding to support developing or expanding these services. To deliver the safest possible care within our existing financial envelope, commissioners will need to agree to remove place based commissioning arrangements so that resources can be deployed where they are most needed.
What we are proposing:
We are proposing to redistribute existing staff and resources so that support for patients is fair, consistent and aligned with need across all localities.
Through our workforce planning, we have identified the size and shape of teams required to prioritise those with the most complex mental health needs, including people requiring intensive rehabilitation support, people with severe affective disorders and those living with complex trauma.
This approach will also help us identify patients who may be better supported by other health and social care partners, including voluntary and community sector organisations.
What this means for patients and staff:
Patients will not see a reduction in service. In areas that have historically been under resourced, people should see improvements in the level and consistency of care. No locality will be left without the staffing levels it needs.
For staff, some colleagues may be asked to work across two neighbouring localities to make best use of skills and resources. Any significant changes will involve engagement and consultation, and we aim to minimise disruption as much as possible.
Benefits of the changes:
These changes will allow us to focus our resources on people with the most complex and enduring mental health needs. This will help us deliver better outcomes, improve safety and provide more consistent support to people who may struggle to access services or present higher levels of risk.
Risks and how we will manage them:
One risk is that staff may feel uncertain about the changes, which could affect workforce stability. We will address this through clear communication, engagement and consultation.
Another risk is that commissioners may not approve the removal of place based arrangements. We will work closely with them to explain why resource redistribution is essential and ensure they understand the needs of this group. The ongoing public inquiry into the Nottingham case may also lead to national commissioning guidance that supports this direction of travel.
Rehabilitation
What the service is and who it helps:
Across Newcastle and Gateshead there are two inpatient rehabilitation services that support adults with serious mental illness and complex needs:
- Elm House (Level 1, community based rehabilitation) in Bensham, Gateshead, with 14 beds for people who need longer term rehabilitation in a community setting.
- Willow View (Level 2, inpatient rehabilitation) at the St Nicholas Hospital site, with 15 beds offering mixed gender accommodation and more intensive rehabilitation.
These services help people rebuild skills, manage their mental health, and move towards greater independence.
Why change is needed:
NHS England guidance describes rehabilitation across two levels: Level 1 community based and Level 2 inpatient based care. We want to make sure our local offer is aligned to this framework, makes best use of specialist inpatient care, and strengthens community support so people can recover closer to home. We are taking a phased approach to reviewing these services (Central locality first, then North, then South) so we can learn as we go and involve people at each step.
What we are proposing:
We are exploring how to modernise our facilities and model of care:
- Willow View refurbishment: We plan to temporarily close Willow View for around three months in 2026/27 to improve the ward environment. During this period we will work to safely discharge or transfer people so care continues. Following refurbishment, Willow View would re open as a dedicated Level 2 inpatient rehabilitation unit for Newcastle and Gateshead, subject to engagement and approvals.
- Elm House future model: With partners, we are developing options for Elm House (currently Level 1). Options include changing its function to support a strengthened community offer with alternative community provision in place and a move from inpatient rehabilitation for Elm House. We are seeking views on what would work best to meet the needs of this patient group and how we change from an inpatient based model for rehabilitation to a more community facing model.
- A community first model: We are keen to design a continuum of support from hospital admission to independent living, with relapse prevention built in to avoid unnecessary readmission. This would be co developed with health and social care commissioners, local authorities, and third sector providers, ensuring future accommodation and care are planned together and rooted in neighbourhoods.
What this means for patients and staff:
For patients, these changes aim to reduce the need for long hospital stays by offering more support in the community. Receiving care closer to home can feel less isolating, help people stay connected to daily life and make it easier to spot early signs of relapse so support can be put in place quickly. A stronger community model also means clearer pathways from inpatient care to supported accommodation and, eventually, independent living.
For staff, any changes would be phased and supported through open engagement, ensuring teams are involved in shaping how services evolve.
Benefits of the changes:
- Safer, more therapeutic inpatient environment at Willow View
- A clearer focus for Level 2 inpatient rehabilitation
- Stronger, more community based pathways that promote independence, reduce hospital stays, and keep care closer to home
- Phased implementation that allows learning and improvement before wider changes
Risks and how we will manage them:
Temporary bed reductions during refurbishment may affect patient flow. We will manage this through careful discharge and transfer planning, close system working, and enhanced relapse prevention and community support. Timelines and impacts will be monitored and shared openly through the consultation process.
In line with the NHS 10-year Plan and its commitment to improve and widen access to care for children and adults needing mental health support. The trust has embedded its single point of access into mental health Urgent Care through the centralised 111 access hub based in Sunderland.
This has enabled work with locally placed based crisis teams to provide timely assessment and evidenced based Home based treatment in line with the national waiting times standards of 4 hour very urgent response and 24 hour urgent response.
The Trust has developed, in collaboration with VCSE, 4 safe havens which provide holistic support and mental health expertise for those in Crisis with a focus on early intervention and prevention. We are around 18 months in to delivering the national pilot 24/7 Mental health hub Hope Haven which offers 4 short stay beds as an alternative to admission and will be using this model as the blue print to delivering 4 additional Neighbourhood Mental health centres over the course of the next 3 years.
The urgent care workforce is under review in relation to supporting us to deliver our model of care with a focus on Urgent Care Assessment across Crisis, Liaison and Health Based places of safety and evidenced based treatment as an alternative to hospital admission.
Access to crisis services
What the service is and who it helps:
CNTW currently provides three services within the urgent care pathway for people who need an emergency or urgent mental health assessment:
- Psychiatric Liaison Teams (PLTs) based in the main acute hospitals in Northumberland, Newcastle, Sunderland and Cumbria. They assess people who arrive at Emergency Departments or who require mental health assessment while admitted to hospital.
- Crisis and Home Based Treatment Teams, offering urgent assessment, support and intensive treatment at home for people experiencing acute mental health distress, helping many avoid admission.
- Health Based Places of Safety (Section 136 suites) in Northumberland, Newcastle, Sunderland and Carlisle. These provide a designated safe environment for individuals detained by police under Section 136 of the Mental Health Act so that they can receive an urgent mental health assessment.
Alongside this, intensive home based treatment is delivered in partnership with service users, families and carers to support people through severe mental health crises in their own homes. This promotes recovery, inclusion and resilience, and helps avoid unnecessary admission.
To make urgent help easier to access, the Trust has also established a single point of access for mental health via the NHS 111 hub in Sunderland. Trained clinicians provide advice, organise assessments, and direct people to the most appropriate support, helping the Trust meet national urgent response standards.
Why change is needed:
While the Trust has already made important improvements to crisis support, including working with voluntary sector partners to open four safe havens that offer early help and holistic support, more change is still needed. We are now around 18 months into running Hope Haven, our 24/7 national pilot Mental Health Hub, which includes four short stay beds as an alternative to hospital admission. These developments represent significant progress, but further expansion is required to ensure people across our Trust footprint who are in crisis receive timely, safe and appropriate support in the right place.
Pressures on the s136 pathway continue to rise: increased detentions, reduced police support, longer lengths of stay due to delays securing inpatient beds, and a growing number of incidents. Staff report feeling overwhelmed, and CQC feedback identified safety concerns, including limited training, lack of fresh-air access, and high levels of anxiety among staff. Between April 2024 and December 2025, 372 incidents were recorded, the highest number occurring at Carleton Clinic.
In response to this the government’s 10 Year Health Plan for England National policy emphasises that A&E settings are unsuitable for people in mental health crisis, and the government’s 10-year plan calls for the development of Mental Health Emergency Departments (MHEDs) and Crisis Assessment Suites.
What we are proposing:
CNTW is proposing a new two site model for s136 provision, with two suites at each site (St Nicholas Hospital, Newcastle and Carleton Clinic, Carlisle), staffed by a dedicated 24/7 specialist team instead of CRHT staff.
Alongside this, three capital bids for new MHEDs across the Trust footprint are currently awaiting confirmation. These MHEDs will link closely with the redesigned s136 model and crisis alternatives. They aim to provide safer, calmer environments, reducing reliance on A&E and supporting the wider shift from hospital based care to community based crisis support.
To support the delivery of these proposals the urgent care workforce is under review to ensure we can deliver our model of care with a focus on Urgent Care Assessment across Crisis, Liaison and Health Based places of safety and evidenced based treatment as an alternative to hospital admission.
Subject to a national bidding process, the learning from Hope Haven will be used as the model for creating four additional Neighbourhood Mental Health Centres across the region over the next three years.
What this means for patients and staff:
For patients:
- Safer, more therapeutic spaces with improved access to outdoor areas.
- Faster, higher quality assessments from a skilled, consistent team.
- New options such as MHEDs, crisis cafés, online safe havens and partner led crisis services offering alternatives to admission.
For staff:
- Reduced pressure on crisis teams, psychiatric liaison staff, and wards.
- A dedicated s136 workforce with enhanced training (PMVA, legal/assessment skills).
- Stronger relationships with police, AMHPs, ED teams and crisis services.
- Benefits of the changes
- Reduction in emergency department attendances as MHEDs divert mental health only emergencies to dedicated, safer environments.
- Improved flow across crisis pathways, reducing 24 hour ED breaches and long ED waits.
- Lower reliance on inpatient admission and shorter hospital stays.
- Capacity freed within crisis teams for home based treatment.
- A more sustainable system that integrates MHEDs, place of safety suites, psychiatric liaison, and crisis alternatives.
Risks and how we will manage them:
Key risks include challenges finding staff without new revenue funding, ensuring medical cover, build timescales, and ensuring full police and AMHP engagement. These will be managed through phased implementation, strong governance, Trust wide workforce planning, and close collaboration with system partners across health, police and local authorities.
Acute admissions inpatient provision
As part of CNTW’s Model of Care, we regularly review staffing levels on our inpatient wards to make sure our workforce is safe, effective and sustainable both now and in the future. Demand for beds continues to rise due to increasing levels of patient need and a higher number of people being detained under the Mental Health Act. These pressures are an important factor in how we plan and improve services.
Two recent developments linked to these pressures include introducing an Enhanced Multi Disciplinary Team (E MDT) approach and expanding access to senior clinical decision makers seven days a week. Funding to support the move to seven day working was secured through the IQPT fund. We are now preparing to move from a voluntary “opt in” system to a formal contractual arrangement so that seven day senior clinical input becomes the standard.
We have also reviewed our staffing levels to ensure they reflect what is needed on a day to day basis. Our “baseline staffing levels” take account of patient numbers, levels of acuity, and the operational tasks required on each ward. These levels are reviewed twice a week to make sure the right staff to patient ratios are in place. Although based on standard working patterns, there is flexibility to respond to changes in clinical need. While these reviews have identified potential efficiencies, we are clear that any changes must not compromise quality of care. We closely monitor service related incidents so we can understand whether staffing changes have any impact.
Alongside staffing levels, we are reviewing the roles of Band 7 and Band 8a clinical staff on our acute inpatient wards. We know that CNTW may be an outlier when compared to similar organisations, and this review will help us establish a more consistent staffing model, remove or realign tasks that do not add value, and support financial sustainability.
Any potential workforce savings from these changes reflect the baseline staffing levels agreed as part of the organisation’s wider financial plan.
In total, there are four key areas of work underway across our acute inpatient wards:
- Developing baseline staffing levels
- Reviewing Band 7 and Band 8a roles
- Introducing the Enhanced MDT model
- Expanding seven day senior clinical leadership
- Together, these changes will help us deliver more consistent care, strengthen safety and quality, and improve the experience of patients and staff. They will also help the Trust meet NHS England expectations around reducing reliance on agency staffing.
We continue to work closely with our Staff Side colleagues throughout this process to ensure staff are informed, supported and able to raise concerns as changes progress.
Older adult inpatient provision
What the service is and who it helps:
CNTW provides three Older Adult inpatient wards at Monkwearmouth Hospital in Sunderland:
- Roker Ward – 12 bed male organic ward
- Mowbray Ward – 12 bed female organic ward
- Cleadon Ward – 18 bed mixed gender functional ward
These wards support older adults with dementia related (organic) needs or severe mental illness (functional). Older Adult Community Treatment Teams provide support, but there is currently no day service provision.
Demand pressures and discharge delays affect the quality and flow of care. Across Roker and Mowbray, a high proportion of people are classed as Clinically Ready for Discharge (CRFD). Over the past six months, around 31%, and more recently 41%, of organic inpatients have been waiting for discharge despite being medically ready. The main reason for delay is the limited availability of suitable community accommodation, including specialist nursing home places. Average delays are 42–45 days, which blocks beds and affects overall patient flow.
There are also financial challenges, with a projected £1.2m overspend for 2025/26, which is not sustainable.
Why change is needed:
The Older Adult pathway is under review due to rising demand, discharge delays, estate limitations and cost pressures. High CRFD levels and slow access to community placements highlight that the current model does not support timely discharge or effective bed utilisation.
The Trust is also working within a wider ICB review of Older Adult mental health services. In addition, the long term “Deciding Together, Delivering Together” strategy will relocate specialist Older Adult services from outdated buildings to refurbished facilities at St Nicholas Hospital, creating a natural opportunity to redesign the inpatient offer.
What we are proposing:
A Steering Group has been set up to explore how best to remodel the organic inpatient pathway. While no decisions have been made, early work suggests the Trust may need to consolidate organic beds into a single 14 bed mixed gender ward, with minor environmental changes to enable this.
The Steering Group is also exploring wider options to support a safe and sustainable model, including:
- a step up/step down service
- intermediate care options
- improving day services provision and how this links with the frailty pathway across our places
- potential development of an EMI nursing home in partnership with local authorities or third sector organisations
- alternatives such as maintaining two wards with reduced bed numbers
The functional ward, Cleadon, is considered too large to offer good therapeutic care and may require a reduction in bed numbers and staffing to ensure balance between quality, safety and financial sustainability.
What this means for patients and staff:
Patients and carers will be invited to share their views during engagement and, if required, through formal consultation. Any changes would aim to improve flow, reduce unnecessary delays and ensure patients receive care in the right setting at the right time.
Staff will be supported through a structured engagement and consultation process (45 days if required). This will include one to one sessions, drop ins and open communication from senior leaders.
Benefits of the changes:
- Better patient flow and more timely discharge
- Reduced CRFD delays and improved length of stay performance
- More sustainable use of beds and workforce
- Modernised, fit for purpose inpatient environments
- Improved financial sustainability for future services
Risks and how we will manage them:
Potential risks include pressure on remaining beds, the possibility of alternative community options becoming blocked, delays to estate timelines, and staffing uncertainty. These will be managed through detailed planning, oversight, engagement with local partners, and a full business case process to ensure safe and effective implementation.
Inpatient provision
What the service is and who it helps:
CNTW has historically provided two specialist Learning Disability inpatient units:
- Rose Lodge in Hebburn, South Tyneside (10 beds) – providing assessment and treatment for adults with significant learning disabilities in a standalone community setting. Its distance from other mental health wards means staff often need higher numbers on shift to safely manage emergencies.
- Edenwood at the Carleton Clinic, Carlisle (6 beds) – providing assessment and treatment for people with learning disabilities who have additional mental health needs, behaviours that challenge, or offending behaviours. This is co located with other inpatient services, enabling closer support.
The demand for these services has changed in line with national policy directives to reduce reliance on inpatient care and transform community services. We also continue to experience people who stay in hospital too long waiting for an appropriate community placement to support transition and discharge into their community.
Why change is needed:
The NHS is changing how inpatient services work for people with a learning disability and autistic people. The aim is to improve quality of care and make sure people get the right support, in the right place, at the right time.
There is a clear direction to:
- Help people stay well in their communities wherever possible
- Reduce long stays in hospital
- Make sure hospital care is only used when it is really needed, and for the shortest time possible
The national priority to transform care and reduce the number of people with a learning disability and autistic people in mental health inpatient settings by developing community alternatives to inpatient care and building the right support for people to live well in their community has made significant progress across the North East and North Cumbria.
Upcoming changes to the Mental Health Act, mean fewer people with a learning disability or autistic people should be detained in hospital. Inpatient stays should be for the shortest time possible and should deliver care in the least restrictive way to support people being discharged as soon as possible to live well in their community, closest to family, friends and vital community support networks.
We are looking to change how specialist inpatient services are used. Currently some people with a learning disability or autistic people receive care and treatment in a one of our mental health wards with specialised reasonable adjustments made for specific needs, for example, this may be environmental adjustments or input from a specialist learning disabilities team.
The aspiration is that a better range of crisis support and community-based services will reduce reliance on inpatient care across all care pathways.
What we are proposing:
We are developing a new service model for people with a learning disability or autistic people who also have mental health needs.
We want to hear views on:
- How we can improve the experience of patients and make sure we’re delivering the best possible care and treatment.
- The Learning Disability In-reach and Transitions Team pilot we have implemented (LDITT – see below) and how we can build on this across our mainstream services.
- Whether a similar in‑reach team can be developed for autistic people.
- How community learning disability services can better support people during a hospital stay and help them return home.
- The best long-term location for specialist inpatient beds for adults with learning disabilities.
Engagement on the long term options include how we sustain community and specialist in reach provision, improve crisis support whilst ensuring we have specialist inpatient services which meet the needs of the local population in terms of their mental health needs.
Scenarios we are considering to develop these options for specialist inpatient provision include:
- Establishing two small units for learning disability provision co-located with other inpatient services (i.e. on a main mental health inpatient site).
- Establishing one specialist inpatient unit for learning disability patients alongside the specialist inpatient autism unit in Morpeth.
- Specialist provision be exclusively provided in the community in the form of independent living spaces to support the needs of this group with our other community partners.
What this means for patients and staff:
Proposals are expected to benefit patients by ensuring that inpatient care is delivered in settings that are better suited to their clinical needs, improving quality, safety and overall experience. For staff, the changes also create opportunities to support moving to a more community facing model whilst ensuring we develop and retain specialist skills for inpatient provision when this is needed.
Formal engagement has already commenced and you can access more information here (LINK).
Benefits of the changes:
- Consistent specialist input through the LDITT
- Improved continuity and safer care
- More efficient use of inpatient beds
- Significant cost savings from operating one unit rather than two
- Strong early feedback from patients, staff and community teams
Risks and how we will manage them:
We recognise that we have to work with our partners to support the system in managing risk and placement breakdown for patients with a learning disability. We also continue to manage the risks and harm caused with patients who remain in hospital who are significantly delayed in terms of their discharge and transition. We must continue with our partners to focus on this in order to ensure we have the right community support in place with independent providers and adult social care.
Community waits for adult ADHD and Autism
What the service is and who it helps:
The Adult ADHD and Autism diagnostic services across the North East and North Cumbria support thousands of adults seeking assessment for neurodevelopmental conditions. Demand has grown rapidly, and waiting lists now exceed 20,000 people across CNTW. The service covers a large geographical footprint and works alongside local mental health teams, primary care, and community providers.
Current challenges include extremely high demand, limited workforce capacity, long waits, and inconsistent referral information. Many referrals lack essential clinical detail, making it difficult to prioritise patients fairly or identify those needing NHS specialist mental health assessment. Without significant change the NHS will not have the capacity to meet demand for this patient group.
Why change is needed:
As a specialist secondary care mental health and learning disability service, it is essential that our clinical resources for patients with ADHD or who are autistic and have mental health needs are prioritised and supported holistically as part of their care needs and treatment plans.
We have wide variation in how patients access services for diagnosis and subsequent treatment. CNTW and Tees Esk and Wear Vallet Foundation Trust have been working together with partners to develop a proposal for a more consistent, fairer approach in line with the regional commissioning intensions.
Nationally, Integrated Care Boards are expected to redesign pathways to ensure people receive the right support from the right provider. This includes expanding the role of accredited providers and strengthening community based options.
What we are proposing:
We propose introducing a region wide re triage process for all adults currently waiting for an ADHD or Autism assessment. This will use a new Patient Self Assessment Tool (PSAT) to gather up to date information on needs and functioning.
Patients will then be directed to:
- NHS specialist services (for those with the highest clinical need or co existing severe mental illness)
- Accredited providers for diagnostic assessments
- Local or neighbourhood support where a diagnostic assessment is not the most appropriate next step
Options considered included continuing the current model, which was rejected due to unsustainability. The preferred model ensures consistency, fairness and better use of limited NHS workforce.
What this means for patients and staff:
Patients will have a clearer pathway, shorter waits over time, and a more appropriate route to support. Many will receive faster assessment or alternative services better matched to their needs.
For staff, the process will require dedicated time for re triage and may involve temporary changes in workload and referral processes. Workforce planning will support this.
Benefits of the changes:
- Fairer and more consistent decision making
- Shorter waits through better prioritisation
- Improved access to community based support
- Stronger focus on those with the greatest clinical need
Risks and how we will manage them:
Risks include workforce pressure, lack of accredited providers, and public concern about pathway changes. These will be managed through clear communication, joint regional planning, and ongoing review of capacity and demand. However, the changes being implemented need to be balanced against the risks of ‘status quo’ and making no changes.
Children and Young People
This plan sets out the work to prioritise the over 20,000 adults waiting for assessment. However, we also must transform the pathway for children and young people. Work has commenced in improving help and support in schools and establishing different pathways for neurodevelopmental needs across the region which will inform what we put in place with our local authority partners. However we know the pace of this is not enough and we will be progressing how we change the pathway and clinical capacity with our commissioners over the next 12 months.
Secure Services and the Northgate site
The overarching vision for the Northgate site is to create a fully utilised, clinically aligned and financially sustainable service footprint.
What the service is and who it helps:
Northgate provides secure mental health services and specialist Learning Disability and Autism (LD&A) support for people across the North East and North Cumbria. It offers a mix of inpatient beds and in reach support for people with complex needs, including those currently placed outside the region. Demand for services is high, some buildings and wards are underused, and parts of the workforce are stretched. There are also people placed out of area for their secure/forensic needs due to limited local bed availability. This affects quality, continuity of care and costs.
Why change is needed:
Evidence shows that too many patients are cared for outside the region (45 people in total, with 31 judged clinically suitable to return home). This impacts patient experience and increases costs for the NHS.
National and regional commissioners are clear that services should:
- Reduce out of area placements
- Strengthen LD&A pathways
- Improve use of NHS estates
- Ensure services are clinically and financially sustainable
Northgate’s current configuration and building usage do not fully support these goals.
What we are proposing:
We are proposing a single, coherent plan for secure and potentially LD&A services at Northgate. Key changes include:
Secure services
- Open and fully utilise all funded secure beds.
- Repatriate out of area patients by June 2026.
- Realign wards to ensure the right bed types are available, including new capacity in Tyne, Elsdon and Linhope wards.
- Identify opportunities for future growth in line with national and regional demand requirements.
Learning Disability and Autism Services
- Create a new LD&A model based at Northgate (subject to engagement and clinical review of the pathway which has commenced)
Estates and workforce
- Ensure no building is left empty and reduce underused floor space to use financial resources well in terms of ‘value for money’.
- Align medical, nursing and therapy staffing with clinical need.
This work will consolidate services at Northgate as this supports repatriation, improves patient flow, strengthens workforce resilience, and avoids costly unused estate.
What this means for patients and staff:
For patients
- More people will receive care closer to home, improving family contact and continuity of care.
- Clearer pathways into, through and out of secure care.
- Modern facilities and a stronger LD&A offer on the Northgate site (subject to ongoing engagement work).
For staff
- Roles may change as services realign.
- Workforce gaps in secure services will reduce through redistribution and new LD&A staffing models.
- Staff will work within more clinically consistent teams.
Benefits of the changes:
- Reduction in out of area placements.
- A clearer, safer, better integrated pathway across secure and LD&A services (subject to engagement).
- More efficient use of buildings and estate.
- A stronger, more resilient workforce model.
Risks and how we will manage them:
Key risks include staffing pressures, delays to estates work, and slower than expected repatriation.
CYP Inpatient Provision – Inpatient Capacity Review
What the service is and who it helps:
This review will be looking at inpatient mental health, learning disability and autism services for children and young people (CYP) across Ferndene and Acklam Road (Lotus Ward). These services support children with complex mental health needs, learning disabilities, autism, and those who sometimes require secure or intensive hospital care. There are currently 34 beds across both sites, covering general admission, learning disability/autism, low secure, psychiatric intensive care (PICU) and medium secure care.
Recent years have seen rising demand, increasing complexity, workforce pressures, and continued use of temporary staffing. Some young people are admitted because crisis support in the community is not strong enough, and Lotus Ward operates separately from the larger Ferndene site, limiting support and flexibility.
Why change is needed:
National policy such as the NHS 10-year Plan and Building the Right Support expects fewer hospital admissions, shorter stays, and more care at home wherever possible. The current model depends too much on inpatient beds, which can disrupt family life, schooling and recovery.
Evidence shows increased need for autism and eating disorder provision, unpredictable demand for general admission beds, safety concerns in some settings, and financial strain linked to high temporary staffing costs. Strengthening community alternatives and ensuring beds are used only when essential will improve outcomes and reduce avoidable admissions.
What we are proposing:
The proposal is to carry out a full review of bed usage, need, and clinical pathways to design a more sustainable, child centred model. This includes:
- Considering changes to the number and type of inpatient beds, including the potential repurposing or reduction of some beds.
- Developing a High Intensity Environment (HIE) by combining low secure and PICU functions, creating a safer and more appropriate setting for the most complex young people.
- Strengthening community based crisis and intensive support to prevent admissions and support earlier discharge.
- A range of options will be explored including doing nothing, reconfiguring beds, and shifting investment into community alternatives, with a preferred model recommended once evidence and engagement are complete.
What this means for patients and staff:
For children and young people:
- More support closer to home and fewer unnecessary hospital stays.
- Inpatient care only where it is clinically essential, with more personalised, trauma informed and developmentally appropriate care.
- Better integration between health, education and social care.
For staff:
- Potential changes to where teams are based and how wards are configured.
- More sustainable staffing models with reduced reliance on temporary staff.
- Opportunities to work in strengthened community and crisis teams.
Benefits of the changes:
- Improved access to the right care in the right place at the right time.
- Reduced admissions and out of area placements.
- Better use of specialist inpatient beds.
- Opportunities to reinvest savings into community based alternatives.
- A clinically and financially sustainable model for the future.
Risks and how we will manage them:
Potential risks include increased pressure on A&E or community services, concerns about access to beds, and challenges during the transition. These will be managed through detailed data analysis, strong clinical oversight, co production with families and staff, and clear mitigation plans for safety, demand, and workforce impact.
Adult Eating Disorder Services
What the service is and who it helps:
Adult Eating Disorder (AED) services support people with serious eating disorders across the North East and North Cumbria. The current model includes inpatient beds, Intensive Day Services (IDS), Intensive support at home and outreach, and specialist community teams offering therapy, physical health monitoring and multi disciplinary support.
There are 20 commissioned inpatient beds across two sites: Ward 31A in Newcastle (closing July 2026) and Birch Ward in Darlington, where most admissions currently take place. IDS services operate Monday to Friday, with no intensive community support at weekends, creating gaps that can lead to avoidable admissions.
Why change is needed:
National policy emphasises reducing inpatient reliance and strengthening community based alternatives. AED services must provide early intervention, minimise restrictive care, and use admission only when clinically essential.
Local evidence shows declining inpatient demand, supported by the expansion of intensive support and strengthened community care. Inpatient occupancy has already reduced over the past two years as a result of community enhancements.
What we are proposing:
This programme will deliver the AED service changes already set out in the Medium Term Financial Plan, based on the reduced need for inpatient care and opportunities to strengthen community treatment.
Key proposals include:
- Reviewing the current two site inpatient configuration, bed usage and occupancy.
- Designing a new regional clinical and operational model, shaped by a full Case for Change, option appraisal and stakeholder engagement.
- Safely reducing reliance on inpatient beds and reinvesting resources into enhanced community and intensive home based treatment.
- Developing modern seven day outpatient and day service models supported by stronger Intensive support at home provision.
The preferred future model will align with national AED service specifications, which prioritise prevention, early intervention and least restrictive care.
What this means for patients and staff:
For patients:
- More support available in their own homes and communities.
- Fewer admissions and shorter stays, with inpatient care remaining available when absolutely necessary.
- More person centred, recovery focused care that helps rebuild confidence, autonomy and resilience.
For staff:
- Changes to inpatient teams as bed numbers and locations evolve.
- Greater emphasis on community based work, requiring new ways of delivering intensive outreach and seven day care.
- Strong clinical leadership and lived experience involvement will guide the transition.
Benefits of the changes:
- Improved recovery outcomes through earlier, community based interventions.
- Reduced need for hospital admission and out of area care.
- More effective use of resources, enabling investment in modern alternatives such as expanded IDS and outreach services.
- A more resilient and sustainable regional AED service that can support more people.
Risks and how we will manage them:
Potential risks include increased pressure on community services, reduced access to beds, or gaps during the transition. These risks will be managed through a structured governance framework with clinical oversight and strong stakeholder engagement.
What happens next
As part of the NHS planning framework the Trust has submitted an overarching plan for the next 3 years. This plan sets out the service changes we have identified to deliver the national policy shifts in the NHS 10 year plan as well as improve the financial sustainability of the Trust.
We will be progressing with specific patient, public, staff and partner engagement on the key service change areas we have identified in this plan, these include but are not limited to:
- Changes proposed to inpatient learning disability provision – alread commenced.
- Changes proposed to Adult Eating Disorders – already commenced.
- Changes proposed to older person’s inpatient provision in Sunderland - to commence May/June 2026.
- Changes proposed to children and young people’s specialist inpatient provision – to commence May/June 2026.
- Changes proposed to rehabilitation services - to commence May/June 2026.
We will continue to inform patients, the public, our staff and our partners on the improvements and developments we have outlined in this plan as they are implemented.